Case history of leprosy
Leprosy has been known since ancient times. Information about the disease was recorded already in the 15th - 10th centuries BC. Leprosy is mentioned in the Bible and the Ebers papyri. Hippocrates described the disease. In ancient times, leprosy was rampant in the east. The widespread spread of the disease was noted in the Middle Ages. At the beginning of the 13th century, epidemics began in Europe. Presumably the disease was brought to this territory by the Crusaders. The deformation of appearance and deformity of leprosy patients caused disgust and fear. Such patients were called “lepers.” They were turned into real outcasts. In order to prevent the spread of infection, many places of settlement for “lepers” were created - leper colonies, where patients were kept until the end of their lives. The first leprosariums were located within the monasteries and contributed to the non-spread of infection, acting as quarantine institutions. In the middle of the 13th century, there were about 19 thousand leper colonies in Europe. Despite the fact that leprosy has been known since ancient times, the causative agent of the disease was discovered by Gerhard Hansen only in 1873. In 1948, the French journalist Raoul Follero founded the Order of Charity, and in 1966 the Federation of European Antileprozoal Associations. January 30th is Leprosy Rights Day.
Henry XIV, Louis XI, the Byzantine Emperor Constantine, and the impressionist artist Paul Gauguin suffered from leprosy.
Rice. 2. Patients with leprosy (“lepers”) were expelled from settlements in ancient times.
Prevalence of the disease
Leprosy is common mainly in countries with tropical climates. The maximum number of patients is recorded in countries such as Brazil, India, Burma, Indonesia, the Philippines, Nepal, Tanzania and the Republic of Congo.
Leprosy in Russia
In the territory of the former USSR, leprosy was recorded in the Lower Volga region, the Far East, Karakalpakia, the North Caucasus, Kazakhstan and the Baltic states. In modern Russia, the disease is rare - isolated cases every year. In total, there are about 700 patients who live in 4 leper colonies located in Astrakhan, Tver, Moscow region and Krasnodar Territory.
Rice. 3. Consequences of leprosy. Loss of fingers.
Treatment methods
Today, leprosy is a curable disease. If the infection is severe, the patient is placed in specialized anti-leprosy institutions. In other cases, the patient receives therapeutic care at home.
For the treatment of leprosy, etiotropic therapy is used. Drug treatment involves the use of sulfone drugs that have an antibacterial effect on Mycobacterium leprae. The most common drugs are “Solusulfone” (it is administered intramuscularly twice a week), “Diaminodiphenylsulfone”, “Sulfametrol”. Dimotsifon is also effective, providing both an antimicrobial and immunomodulatory effect.
Broad-spectrum antibiotics (Rifampicin, Ofloxacin), vitamins, and hepatoprotectors are also prescribed. Due to a decrease in the body's protective functions, there is a high probability of developing tuberculosis, so patients are often prescribed unscheduled BCG vaccination.
To prevent disability, physiotherapeutic procedures are recommended: massage, electrophoresis, UHF, therapeutic and preventive gymnastics and physical education. In order to prevent orthopedic diseases, it is recommended to wear special aids (insoles, ties, staples, bandages and orthoses).
The causative agent of leprosy. Microbiology
Despite the fact that leprosy has been known since ancient times, the causative agent of the disease was first discovered by the Norwegian scientist Gerhard Hansen only in 1873.
Taxonomy of the pathogen
The cause of leprosy turned out to be a bacterium (bacillus) belonging to the Mycobacteriacea family, called Mycobacterium Leprae hominis (Hansen's bacillus, Hansen's bacillus).
In 2008, a second type of bacterium that causes leprosy, Mycobacterium lepromatosis, was discovered. These bacteria have been found to cause diffuse lepromatous leprosy, prevalent mainly in the Caribbean. The disease is characterized by extensive ulcerations on the skin, damage to nerves and internal organs.
The structure of the causative agent of leprosy
Mycobacterium leprosy is similar to tuberculosis bacilli in a number of ways.
- The bacteria are cylindrical in shape. Straight or slightly curved. Their length ranges from 1 to 8 microns, width - from 0.3 to 0.5 microns. The ends are rounded or slightly pointed.
- They are located singly or in clusters, resembling cigarette packs or balls (leptospirosis balls). Motionless.
- The causative agents of leprosy do not form spores.
- Bacteria are obligate intracellular parasites. They are ingested by macrophages, but are not digested (incomplete phagocytosis).
- Pathogens have the property of pleocytosis (diversity of forms). In leprosy you can find granular, club-shaped, budding, branched, filamentous, coccoid and dumbbell-shaped forms of bacteria.
- The cytoplasm of mycobacteria is surrounded by several membranes:
- the first (innermost) shell is represented by a three-layer cytoplasmic membrane, which includes lipoprotein complexes and enzyme systems;
- Next is the cell wall, which ensures the stability of the shape and size of the pathogen and provides mechanical, chemical and osmotic protection. The wall contains lipids, mycolic and leprosic acids, and wax (leprosin). Its thickness is 3 - 10 nm;
- A microcapsule is closely associated with the cell wall - the outermost wall, which is a polysaccharide shell, consists of 3 - 4 layers, its thickness is 5 - 10 nm. The microcapsule protects the cell from the effects of negative environmental factors.
Rice. 4. Mycobacteria leprosy are cylindrical, straight or slightly curved.
Pathogenicity factors
The virulence factor of Mycobacterium Leprae is the phosphatide fraction, which is part of the cell wall lipids.
Antigens of the causative agent of leprosy
The microcapsule of the leprosy bacterium has antigenic properties. Two antigens have been identified: heat-stable and heat-labile. The heat-stable antigen (polysaccharide) is common to all mycobacteria; the heat-labile antigen (protein) is highly specific for leprosy mycobacteria.
Pathogen genome
The genome of the causative agent of leprosy was first deciphered in 2001. It consists of 3,268,203 nucleotide base pairs. Genetics from the University of Tübingen (Germany) have proven that the genome of Mycobacterium leprae has not changed over the past 500 years.
Reproduction
Mycobacterium leprosy reproduces by transverse fission. The process of reproduction occurs only in the cytoplasm of tissue cells.
Sustainability
In the external environment, leprosy pathogens exhibit increased resistance, but at the same time their virulent properties are quickly lost.
Microscopy
According to Ziehl-Neelsen, mycobacteria leprae are stained pink (Gram-positive, acid-fast). In recent years, the technique of staining smears using the Marcinowski method has become widespread.
Cultivation
It is not possible to grow Mycobacterium Leprae on artificial media. For cultivation, special media are used that contain human serum. In vitro, lineages of isolated mycobacteria are maintained in armadillos and on the paws of infected mice.
Rice. 5. The causative agents of leprosy (Mycobacterium Leprae) are located singly or in clusters, reminiscent of cigarette packs or balloons.
Complications of leprosy
Other complications include visual impairment and complete blindness, mutilation, finger deformation, and the development of contractures. Due to the fact that leprosy affects the nervous system, paralysis begins. Granulomas that form on the face cause a deformity called “lion face,” while granulomas on the bones and joints lead to brittle bones and disability. And formations on internal organs lead to diseases such as: pneumonia, hepatitis, pyelonephritis, nephritis, lymphadenitis. If the disease is advanced, it can be fatal.
Epidemiology
Leprosy is a low-contagious disease. When infected, the disease develops in 10 - 20% of cases. There is a high natural resistance to leprosy infection. A strong immune system guarantees that a person will not get leprosy.
Risk group
Those at high risk for leprosy include those living in endemic areas. There is a high risk of getting sick among armadillo hunters, those who make crafts from the animals' shells, and when eating animal meat. Living in unsanitary conditions, malnutrition, alcoholism, hard physical labor, and diseases that weaken the immune system contribute to the disease. Leprosy is common in economically underdeveloped countries among the poorest segments of the population.
Source of infection
The reservoir and source of leprosy pathogens is a sick person and the armadillo animal. A person becomes infected from an animal through scratches received while hunting or by eating meat. Armadillos live in Central and South America and belong to the class of mammals. Every year, up to 150 people become ill with leprosy in the United States. All of them either hunted armadillos, or ate their meat, or made fakes from the armor of the animals.
How is leprosy transmitted?
Airborne droplets and contact are the main routes of transmission. The disease is not transmitted in utero.
- A sick person who is not undergoing treatment spreads Mycobacterium leprosy by coughing and sneezing. When talking, bacteria spread within a radius of up to 1.5 meters.
- Somewhat less frequently, pathogens enter the human body by contact through microcracks, scratches, wounds or scratches. The patient's belongings are also a factor in the transmission of infection. Mycobacterium leprosy in patients during periods of exacerbation is found in urine, tears, semen, urethral discharge, blood and breast milk.
Rice. 6. The photo shows an armadillo. The animal has a shell consisting of horny scutes, movably connected to each other.
Reasons for development
The causative agent of leprosy was discovered in 1874 by the Norwegian scientist Gerhard Hansen.
Mycobacterium leprae is a gram-positive bacteria that belongs to intracellular parasites, the morphological properties of which are highly similar to Koch's bacillus (causes tuberculosis).
Transmission routes
Contrary to popular belief, leprosy is not very contagious.
The source of infection is sick people. The bacillus is excreted in nasal mucus, feces, urine, and saliva; Leprosy also releases bacilli from the ulcerated surface into the environment. Infection most often occurs through direct skin contact (mycobacteria penetrates through microcracks or wounds). Also, transmission of the disease can occur through kissing, sexual intercourse or bites of blood-sucking insects. It is also believed that the infection can be transmitted through a patient's cough.
People with strong immune systems are resistant to leprosy. The disease in this case is less contagious and infection can occur only through prolonged close contact. The incubation period (the time from infection to the appearance of the first signs) lasts on average from three to seven years.
Pathogenesis
Leprosy pathogens enter the human body through the mucous membrane of the upper respiratory tract and damaged skin. The full picture of the disease develops after an incubation period of years or decades. The penetration of Mycobacterium leprosy into the human body causes disease only in 10 - 20% of cases.
Lepromatous granulomas
Mycobacteria affect the skin, mucous membranes, superficially located peripheral nerves and internal organs, where granulomas form. In the lepromatous type of leprosy, granulomas consist of foamy macrophages stuffed with mycobacteria. Clusters of granulomas form lepromas. In the tuberculoid type of leprosy, granulomas consist of epithelioid cells and contain a small number of pathogens.
Rice. 7. Patients with leprosy. Lepromatous granulomas are visible on the face and neck.
Lepromatous neuritis
Leprosy affects the peripheral nervous system. There is a pronounced tropism of pathogens for lemmocytes - Schwann cells, located along the axons of nerve cells (long process), which perform supporting and trophic functions. Inflammation of peripheral nerves and associated neurological disorders develop more quickly in the tuberculoid type. In lepromatous leprosy, peripheral nerves are affected late. Lepromatous neuritis has an ascending nature. Gradually, the nerve fibers are destroyed and replaced by connective tissue. Damage to peripheral nerves leads to the development of motor and trophic disorders.
Rice. 8. Damage to peripheral nerves. Claw-shaped brush.
Damage to internal organs
More pronounced inflammation of internal organs is observed in the lepromatous type of leprosy. In the mucous membrane of the upper respiratory tract, lymph nodes, liver, spleen, testicles, adrenal glands, kidneys, heart, lungs, granulomas appear, consisting of macrophages filled with a huge number of leprosy pathogens.
Types of leprosy
Depending on the degree of immunological reactivity (cellular immunity), the patient develops one or another type of leprosy.
- The tuberculoid type of leprosy (the most favorable) is formed in individuals with a high degree of immunological reactivity. The disease is less dangerous for others. The course is not severe, with primary damage to the skin and peripheral nerves. The rashes on the skin look like small papules and are accompanied by anesthesia. The infiltrates contain a small number of pathogens.
- The lepromatous type of leprosy occurs in individuals with a low degree of immunological reactivity. Antibodies produced during illness do not protect the body from infection. The disease affects the skin and mucous membranes, nerve trunks, lymph nodes and internal organs. Leproma infiltrates contain a huge number of mycobacteria. Over time, lepromas disintegrate. The resulting ulcers heal slowly. The lepromatous type of leprosy may have blurred and atypical forms.
- The undifferentiated type of leprosy develops when the type of immunological activity has not yet been formed in patients. With a favorable course, the tuberculoid type of leprosy develops in the future; with a low degree of immunological reactivity, the lepromatous type of leprosy develops.
Rice. 9. Tuberculoid (photo on the left) and lepromatous (photo on the right) type of leprosy.
What do lepers look like?
Lepers are people with leprosy (leprosy) or chronic granulomatosis. Since the disease has been known since the times of the Old Testament, it is not surprising that methods of treating and avoiding this disease began a very long time ago. The attitude of healthy people towards lepers has always been the same - people try to avoid contact with the sick so as not to contract the infection. However, modern medical knowledge helps to avoid cruel methods.
How lepers were treated, then and now:
- In ancient times, lepers were subjected to severe persecution. They were expelled from the settlements, their homes and belongings were destroyed by burning. A leper (outcast) had to avoid contact with healthy people, wear torn clothes and not cover his head, and those with leprosy were also forbidden to create families. Thus, lepers became outcasts and wretched.
- In the Middle Ages, during the leprosy epidemic, leper colonies began to be organized - settlements for patients and their families. The creation of leper colonies meant clinics where lepers would undergo treatment. In fact, the patients were placed in strict quarantine, where contact with lepers was only limited in a closed area. Since no treatment was provided, and contact with infected people was not interrupted, the sick only lived out their days.
- Modern science has discovered almost everything about leprosy. One such knowledge is the fact that leprosy is not transmitted by light touch to the patient, and does not always lead to death. It is also known that 93-95% of the world's population have strong immunity to infection, and there is no risk of infection for them. Having this information, people no longer react so violently to infected patients, although there is inner fear in everyone.
Nowadays, drug treatment of lepers is carried out quite successfully. Depending on the treatment, it takes place in a specialized infectious diseases hospital, and after the course of treatment they must undergo regular medical examination.
In cases where the disease is detected at an early stage, positive treatment results can be expected within 2-3 years; in more advanced stages, treatment can take decades. You should also know that characteristic external signs can also occur in other pathologies: leishmaniasis, tertiary syphilis, toxicerma, tuberculosis and sarcoidosis of the skin, erythema nodosum and erythema multiforme.
There is a fairly quick and simple method for diagnosing leprosy (it may not be accurate): inject 1 ml of a 1% solution of nicotinic acid into the area of the leprosy rash; if the result is positive, within 3 minutes swelling and redness will appear at the site of the rash. For a more accurate result, it is necessary to undergo a full diagnosis.
Lepromatous type. Signs and symptoms
The lepromatous type of leprosy is characterized by the development of various elements of skin lesions - fuzzy spots, plaques, infiltrates and nodes. When the disease occurs, the mucous membranes and internal organs are involved in the pathological process quite early, and the nervous system quite late. This type of leprosy is difficult to treat. A huge number of pathogens are localized in the elements of skin lesions. The lepromine reaction is negative due to the developed anergy.
Leprosy skin lesions
The disease most often affects the skin of the face, ears, wrists, elbows, knees and buttocks. Lepromas appear extremely rarely on the scalp, inner parts of the eyelids, armpits, elbows and popliteal fossae.
Spots and plaques
At the beginning of the disease, barely noticeable, blurred, reddish spots appear on the skin, transforming into plaques. Plaques do not have clear boundaries. Over time, as a result of the development of vascular paresis and hemosiderosis, spots and plaques acquire a brown or copper (rusty) tint. Due to increased sebum secretion, their surface becomes smooth, shiny, glossy (greasy). Enlarged excretory ducts of sweat glands and vellus hair follicles in the area of infiltrates give the skin an “orange peel” appearance. Over time, sweating decreases and stops altogether. Sensitivity in the affected areas is not impaired. After 3 - 5 years, spots and plaques transform into lepromas.
Lepromas
Initially, lepromas resemble small single or multiple dense nodules ranging in size from 1 - 2 mm to 2 - 3 cm, painless, with a greasy surface, sharply demarcated from the surrounding tissues, and contain many leprosy pathogens. Over time, the tubercles transform into powerful infiltrates - nodes. Lepromas are dermal and hypodermal.
Hypodermal lepromas are located under the dermis (the skin itself) and at first the diseases are detected only by palpation. When they reach the dermis they become visible to the eye.
Dermal lepromas initially look like oval-shaped papules, gradually turning into bumps that have a reddish-rusty color, with a shiny surface, and rise above the surface of the skin.
Sometimes lepromas resolve. A pigmented spot remains in their place. Sometimes lepromas ulcerate. The formation of ulcers occurs from the center. They have steep, steep, raised edges. The bottom of the ulcers is covered with a yellowish-gray coating. Ulcers can merge to form extensive ulcerative surfaces. The bloody discharge contains a huge number of mycobacteria (up to 1 billion per 1 cm3). Gradually the ulcers scar. In their place, a sunken (sometimes keloid) scar remains. When ulceration of deep-lying lepromas occurs, joints and small bones are involved in the pathological process, which are destroyed and fall off (mutilatio), leading to deformities and disfigurement.
Signs and symptoms of leprosy affecting the face
Diffuse infiltration of facial skin leads to deepening of natural wrinkles and folds. The brow ridges begin to protrude sharply forward. The earlobes are growing. The nose, lips, cheeks and chin thicken. They take on a lobed appearance and a fierce expression, reminiscent of a “lion's face” (fades leonina).
Rice. 10. Photos of people suffering from leprosy. Multiple lepromas are visible on the skin of the face.
Signs and symptoms of leprosy with nasal lesions
The nasal mucosa is always affected in leprosy and long before the skin is affected. Rhinitis and nosebleeds are the first signs of leprosy. The nasal mucosa turns red and swells, then small erosions appear and massive crusts form, which leads to difficulty breathing. A picture of leprosy rhinitis develops.
Leprosy ulceration leads to destruction of the nasal septum. First, the tip of the nose rises upward, then the nose sinks (“saddle nose”).
Mycobacterium leprosy is detected in mucosal staples. Especially many pathogens are localized in the mucous membrane of the cartilaginous part of the septum.
Rice. 11. People suffering from lepromatous leprosy were called lepers. The photo shows patients whose faces are disfigured by leprosy.
Signs and symptoms of leprosy in the mouth
In severe leprosy, damage to the mucous membrane of the oral cavity and larynx is noted. The soft and hard palate, the back of the tongue and the red border of the lips are affected.
Damage to the vocal cords and epiglottis leads to a narrowing of the glottis and aphonia (loss of sonority of the voice).
Rice. 12. With leprosy, the earlobes grow.
Signs and symptoms of leprosy in the eyes
With lepromatous leprosy, the organs of vision are often affected: the episclera becomes inflamed (episcleritis), the cornea of the eye (focal keratitis), the iris (iridocyclitis), the outer layer of the eye (conjunctivitis), clouding of the lens is noted, and the edges of the eyelids become inflamed.
The appearance of lepromas on the surface of the iris leads to disruption of accommodation and deformation of the pupil. Lepronose keratitis and iridocyclitis without treatment lead to complete loss of vision. When the edges of the eyelids become inflamed, eyelashes fall out. Leprosy keratitis is characterized by the absence of discharge and mild symptoms of inflammation.
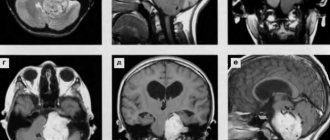
Rice. 13. Damage to the organs of vision due to leprosy.
Damage to hair and nails due to leprosy
After 3 - 5 years from the onset of the disease, hair loss is observed in areas of infiltration. Hair falls out from the eyebrows, eyelashes, beard and mustache areas. On the eyebrows, hair begins to fall out from the outer edge. In areas of infiltration, vellus hair loss is noted.
Nails with leprosy lose their shine, become dull, thickened, brittle, and acquire a grayish tint.
Rice. 14. As a result of trophic disorders in leprosy, mutilation (rejection) of the hands and feet develops.
Signs and symptoms of leprosy affecting internal organs
In lepromatous leprosy, damage to internal organs is noted.
- The liver and spleen increase in size and become denser. Many millet-like lepromas appear in the tissues of these organs. Chronic hepatitis develops.
- All groups of lymph nodes (except for the thoracic and mesenteric ones) are enlarged. They acquire a dense consistency, are mobile and painless.
- Leprosy affects the endocrine glands. A person ages quickly. Women experience menstrual irregularities and early menopause. In men, the testicles (orchitis) and appendages (epididymitis) are affected. Testicular function decreases. The sclerotic process leads to azospermia. Gynecomastia and infantilism develop. Potency decreases to the point of impotence.
Rice. 15. With atrophy of the circular muscles, the eyes do not close completely.
Signs and symptoms of leprosy affecting the nervous system
In leprosy, the peripheral nervous system is affected late. This is due to the high resistance of the axial cylinders to lepromatous infection. Basically, patients develop symmetrical polyneuritis. Nerve trunks affected by infection thicken, become dense and smooth, and are easily palpated.
In areas where leprosy infiltrates develop, sensitivity persists for a long time, but is lost over time until complete anesthesia is achieved, which leads to frequent burns and injuries that patients do not notice. Its causes are compression of the nerves by cellular infiltrates.
Deep sensitivity, periosteal and tendon reflexes are preserved.
When the central nervous system is damaged, neuroses and psychoses develop.
When the peripheral nervous system is damaged, patients with leprosy develop motor and trophic disorders, and sensitivity is impaired.
Trophic disorders:
- Skin pigmentation is disrupted.
- Trophic ulcers appear on the feet.
- Mutilation (rejection) of the hands and feet is noted. At first, the hands and feet become soft, like the legs of frogs or seals, and then spontaneously tear off. The hands and feet are shortened.
- The function of the sweat and sebaceous glands is impaired. Over time, hypofunction is replaced by a complete absence of sweating and sebum secretion. The skin becomes rough and further cracks.
Movement disorders:
- As a result of the predominance of flexor tone, contractures develop. The fingers and toes bend (claw-shaped hand, cauda equina).
- As a result of muscle atrophy, the interosseous spaces collapse. The hand becomes flattened and resembles a monkey's paw.
- With atrophy of the orbicularis muscles, the eyes cannot close completely (lagophthalmos).
- Damage to the facial nerve leads to atrophy of the facial muscles. The face becomes mask-like and takes on a sad expression.
- With the disease, paresis of the masticatory muscles develops.
Rice. 16. Consequences of leprosy. When the nervous system is damaged, contractures, muscle atrophy and trophic disorders develop.
Treatment and prevention of leprosy (leprosy)
Treatment is a long-term course (up to 3-3.5 years) with the prescription of anti-leprosy drugs of the sulfone group (diaphenylsulfone, solusulfone, diucifone, etc.). The duration of the course is 6 months, the break in treatment is 1 month. Multibacterial leprosy requires initial administration of rifampicin, dapsone or clofazimine, after which switching to sulfone group drugs. Evaluation of the effectiveness of treatment is controlled by bacterioscopic and histological research methods. Currently, there are 4 leper colonies in Russia (a place for detection, treatment, isolation, and prevention of leprosy): in Astrakhan, Krasnodar Territory, Sergiev Posad District of the Moscow Region, Stavropol Territory.
The main problem of WHO is the fight against leprosy at the level of primary prevention. Today, the main goal should be early diagnosis and effective drug therapy. Secondary prevention measures—identifying cases of the disease—are also important. This can be achieved through primary health care with the active participation of the entire population of a country where cases of leprosy have been reported. In places where leprosy is endemic, mass surveys of the population, sanitary and educational work among the population and doctors are carried out. In addition to the epidemiological situation, socio-economic factors are of great importance, which explains the widespread spread of the disease among the poorest populations in Asia and Africa. The health systems of these countries prioritize expanding services to identify and treat leprosy patients and ensure that modern treatment is available to all patients. Prevention of leprosy among medical personnel and other persons who, by the nature of their work, come into contact with patients, consists of strict adherence to sanitary and hygienic rules (frequent hand washing with soap, mandatory sanitation of microtraumas, etc.). Cases of infection of medical personnel are rare.
medlibera.ru
Signs and symptoms of leprosy. Tuberculoid type
Tuberculoid leprosy is relatively benign and slow. The disease affects the skin and peripheral nerves. Internal organs are slightly affected. Cases of spontaneous regression are often observed. In most cases, the prognosis of the disease is favorable. Tuberculoid leprosy has a low degree of contagiousness.
Skin lesions
In the tuberculoid form of the disease, depigmented or reddish spots with central blanching and sharply defined boundaries appear on the skin. The spots increase in size over time, and their edges rise. Along the edges of the spots there are dense and flat papules, delimiting the damaged area from healthy skin. When spots merge on the skin, patterns of a bizarre ring-shaped configuration are formed. The central part of the spots undergoes depigmentation and atrophy, and fades over time. Within the affected area, there is no skin sensitivity, sweating and sebum secretion stops. The resulting injuries, damage and burns lead to the development of secondary flora.
Rice. 17. Tuberculoid leprosy.
Damage to the peripheral nerves develops in the same way as in the lepromatous form of the disease, but already in the first stages of the disease and more easily. The affected nerve trunks (usually the radial, ulnar, facial and parotid nerves) become painful over time, thicken and begin to be palpated. Contractures and muscle atrophy develop, causing the limbs and face to take on a characteristic appearance (mask-like face, claw-shaped hand, horse foot). The skin appendages are affected - the work of the sebaceous and sweat glands is disrupted, hair and eyelashes fall out, nails thicken and crumble. The lepromine reaction is sharply positive.
Rice. 18. Tuberculoid type of leprosy.
How is leprosy transmitted?
All prohibitions against lepers were based on the opinion that leprosy is very easily transmitted from an infected person to a healthy person, both by touch and through the air.
With the development of medicine, it turned out that in fact, leprosy is not so easily transmitted. This disease is not particularly infectious, and it takes a long time to transmit the disease through physical contact. Simply put, leprosy is not transmitted through handshakes
.
The disease can be transmitted through droplets secreted from the nose and mouth of a leprosy patient, as well as through frequent contact with lepers who are not receiving treatment.
It is worth noting that different types of disease have different degrees of transmission. Thus, tuberculoid leprosy is forty times less contagious than lepromatous leprosy. According to some doctors, most people have sufficient immune protection and only 10% of the population is vulnerable to the disease.
Undifferentiated type of leprosy
The undifferentiated (borderline) type of leprosy develops when the patient has not yet developed a type of immunological activity. With a favorable course, the tuberculoid type of leprosy subsequently develops; with a low degree of immunological reactivity, the lepromatous type of leprosy develops. The lepromine reaction, depending on the direction of the pathological process, can be negative or positive. The undifferentiated (borderline) type of leprosy combines the clinical manifestations of 2 main types of the disease, but with a milder course.
Rice. 19. The undifferentiated (borderline) type of leprosy develops in cases where the type of immunological activity has not yet formed.
Disease prevention
There is no vaccine against leprosy. There is an opinion that the BCG vaccination also protects against leprosy infection, but there is no data to support this assumption.
Therefore, disease prevention is aimed at improving living conditions, improving the quality of life, and strengthening the immune system.
Those infected with leprosy must use separate utensils, their own personal hygiene items, and promptly treat wounds. Particular attention to personal hygiene should be paid to persons in contact with infected people.
Relatives of a person with leprosy must take a lepromin test, be constantly under the supervision of a doctor, and promptly follow his recommendations.
Gerhard Hansen and Raoul Follero
Two people played a significant role in the history of this disease. Gerhard Hansen, a Norwegian physician, is famous for discovering the causative agent of leprosy in 1873. He announced the discovery of Mycobacterium leprae in the tissues of all patients, but he did not recognize them as bacteria and received little support from his colleagues. Later it turned out that mycobacteria leprosy are similar in their properties to tuberculosis, but are not capable of growth on artificial nutrient media, which made it difficult to study leprosy.
Source: aif.ru (Arguments and Facts)