This term has other meanings, see Stomach (meanings).
The request for "stomach" is redirected here. A separate article is needed on this topic.
Stomach
(Latin
ventriculus
, Greek gaster) - a hollow muscular organ, part of the digestive tract, lies between the esophagus and the duodenum.
The volume of an empty stomach is about 0.5. After eating, it usually stretches to 1 liter, but can increase to 4 liters.
The size of the stomach varies depending on the body type and degree of filling. A moderately full stomach has a length of 24-26 cm, the greatest distance between the greater and lesser curvature is no more than 10-12 cm, and the front and rear walls are separated from each other by 8-9 cm. An empty stomach has a length of 18-20 cm, and the distance between the greater and lesser curvature - 7-8 cm.
Content
- 1 Gastric ligaments
- 2 Functions of the stomach
- 3 Development of the stomach
- 4 Anatomical characteristics 4.1 Topography of the stomach 4.1.1 Skeletotopy of the stomach
- 4.1.2 Syntopy of the stomach
- 4.1.3 Holotopy of the stomach
- 5.1 Mucosa 5.1.1 Epithelium
- 5.1.3.1 Submucosa
Digestive organ - what is it?
The human stomach is an elastic “tool”, a pouch-like extension of the digestive tract that can fit between the esophagus and the intestines. Food is collected in it, digested, turning from a solid state into a mushy state, undergoing treatment with digestive juice. The anatomy of the human stomach includes information about its purpose, structure, pathological signs and treatment.
Purpose and functions of the stomach in humans
The physiology of the stomach consists of accumulation and mixing of the coma, including partial separation of proteins. This function facilitates the gastric process. In addition, there are other, no less important morphological mechanisms:
- food safety;
- basal secretion of gastric juice is regulated;
- chemical food processing;
- movement of food and timely emptying;
- blood absorption of nutrients;
- providing a bactericidal effect;
- protective functions;
- removal of metabolic products;
- separation of substances whose action affects the functioning of the endocrine glands.
Gastric ligaments
The peritoneal ligaments of the stomach from the lesser curvature side belong to the lesser omentum
u.
Hepatogastric ligament, lig. hepatogastricum
, which is a continuation to the left of the hepatoduodenal ligament, approaches the pyloric part and the lesser curvature of the stomach from the porta hepatis. Here its anterior and posterior leaves pass to the corresponding walls of the stomach.
On the side of the greater curvature of the stomach are the ligaments that make up the greater omentum.
Gastrophrenic ligament, lig. gastrophrenicum
, passes from the diaphragm to the bottom of the stomach.
Gastrosplenic ligament, lig. gastrosplenicum
from the upper part of the greater curvature it approaches the hilum of the spleen.
Gastrocolic ligament, lig. gastrocolicum
, connects the greater curvature of the stomach with the transverse colon from the pylorus to the lower pole of the spleen. It is loosely connected to the anterior wall of the transverse colon, which allows bloodless separation of the greater curvature of the stomach along with the greater omentum from the transverse colon during gastric resection for cancer.
The listed ligaments of the stomach are often called superficial.
Definition of disease
The main difference between pharyngitis is damage to the larynx. Translated from Latin, pharynx is designated by the word “pharynx,” which gives the name to the disease. The ending with “itis” indicates an acute inflammatory process. Therefore, pharyngitis is not a simple difficulty swallowing or irritation of the back of the throat, but a serious condition that must be treated with the help of doctors. Pharyngitis is very similar to the similar disease tonsillitis, but if you study these pathologies in more detail, significant differences can be identified between them.
With tonsillitis, the side walls become inflamed, and pharyngitis most often occurs only with damage to the back wall of the throat. This type of disease cannot be treated carelessly. If treatment is not started in time, the entire body may suffer from complications. Therefore, when the first signs of pharyngitis appear, you should immediately go to an appointment with an otolaryngologist. An experienced specialist will always determine the type of disease and prescribe the appropriate treatment regimen. You should not try to identify the disease yourself, much less treat it. All manipulations, and especially traditional methods of treatment, must be agreed with a doctor.
Functions of the stomach
- accumulation of food mass, its mechanical processing and promotion into the intestines;
- chemical processing of food mass using gastric juice (1-2.5 l/day) containing enzymes (pepsin, chymosin, lipase) and hydrochloric acid;
- secretion of the antianemic Castle factor (in the mid-20th century it was noted that anemia occurs after gastric resection), which promotes the absorption of vitamin B12 from food;
- absorption of a number of substances (water, salt, sugar, etc.);
- excretory (increased with renal failure);
- protective (bactericidal) - due to hydrochloric acid;
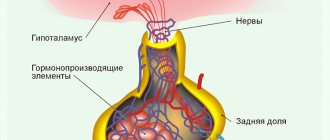
- endocrine - the production of a number of hormones and biologically active substances (gastrin, motilin, somatostatin, histamine, serotonin, substance P, etc.).
Treatment and preventive measures
Treatment of most pathologies occurs exclusively through surgery. Thus, when diagnosing a congenital diverticulum, resection is necessarily prescribed. The same operation is performed if a choristoma (accessory pancreas) or a hollow formation is detected. It is removed completely, sometimes with partial resection of the stomach. For pyloric stenosis, doctors perform a pylorotomy. But Menetrier's disease (chronic hypertrophic polyadenomatous gastritis) most often does not require surgery, but the patient is constantly under medical supervision.
If a patient’s stomach pathology is accompanied by additional problems with the organs, a treatment and recovery strategy is prescribed individually after diagnosis and consultation with the attending physician.
Prevention of any pathologies is possible only during pregnancy. It is important to carefully monitor diet and lifestyle, and then gastric malformations will not affect the fetus. In the case of hereditary diseases, medical genetic counseling is mandatory. As for recovery after treatment, the prognosis is mostly positive. The survival rate of patients with congenital pyloric stenosis and atresia is 95% if treatment was provided in a timely and professional manner.
Stomach development
Develops from the anterior part of the trunk part of the foregut.
At 5-6 weeks, differentiation of the intestinal tube occurs: a fusiform expansion appears, which is suspended on the ventral and dorsal mesenteries. The omental bursa begins to form. In the area of greater curvature, increased growth of the dorsal mesentery occurs.
At 7-8 weeks, the foregut in the stomach (caudal end) makes turns: around a vertical axis from left to right (the right wall becomes posterior, the left - anterior) and around the sagittal axis from bottom to top (the lesser curvature turns upward, the greater - downward). The ventral and dorsal mesenteries atrophy.
At 9-10 weeks the stomach tissues differentiate, and at the end of 3 months the stomach is formed.
Anatomy of the gastrointestinal tract (GIT)
Digestive system
is a human organ system consisting of the digestive or gastrointestinal tract (GIT), liver and pancreas, designed to process food, extract nutrients from it, absorb them into the blood and excrete undigested residues from the body.
Anatomy of the gastrointestinal tract (GIT)
Between the absorption of food and the eruption of undigested residues from the body, an average of 24 to 48 hours passes. The distance that the food bolus covers during this time, moving along the digestive tract, varies from 6 to 8 meters, depending on the individual characteristics of the person.
Oral cavity and pharynx
Oral cavity
is the beginning of the digestive tract.
In front it is limited by the lips, above by the hard and soft palate, below by the tongue and sublingual space, and on the sides by the cheeks. Through the pharynx (isthmus of the pharynx), the oral cavity communicates with the pharynx. The inner surface of the oral cavity, as well as other parts of the digestive tract, is covered with a mucous membrane, onto the surface of which a large number of salivary gland ducts emerge.
The lower part of the soft palate and arches are formed mainly by the muscles involved in the act of swallowing.
Language
- a mobile muscular organ located in the oral cavity and facilitating the processes of chewing food, swallowing, and sucking. The tongue is divided into body, apex, root and back.
From above, from the sides and partially from below, the tongue is covered with a mucous membrane, which fuses with its muscle fibers and contains glands and nerve endings that serve for the sense of taste and touch. On the back and body of the tongue, the mucous membrane is rough due to the large number of papillae of the tongue, which precisely recognize the taste of food.
Those located at the tip of the tongue are tuned to perceive sweet taste, those at the root - bitter, and sour taste is recognized by the papillae on the middle and lateral surfaces of the tongue.
From the lower surface of the tongue to the gums of the lower front teeth there is a fold of mucous membrane called the frenulum. On either side of it, at the bottom of the mouth, the ducts of the submandibular and sublingual salivary glands open. The excretory duct of the third, parotid salivary gland, opens in the vestibule of the mouth on the mucous membrane of the cheek, at the level of the upper second molar.
Pharynx
- a muscular tube 12-15 centimeters long connecting the oral cavity with the esophagus, located behind the larynx and consists of 3 parts: the nasopharynx, oropharynx and laryngeal part, which is located from the upper border of the laryngeal cartilage (epiglottis), which closes the entrance to the respiratory tract during swallowing , to the entrance to the esophagus.
Esophagus
Esophagus
, connecting the pharynx with the stomach, is located behind the trachea - the cervical region, behind the heart - the thoracic region and behind the left lobe of the liver - the abdominal region.
The esophagus is a soft elastic tube about 25 centimeters long, which has 3 narrowings: upper, middle (aortic) and lower, and ensures the movement of food from the oral cavity to the stomach.
The esophagus begins at the level of the 6th cervical vertebra in the back (cricoid cartilage in the front), at the level of the 10th thoracic vertebra it passes through the esophageal opening of the diaphragm, and then passes into the stomach.
The wall of the esophagus is capable of stretching as the bolus passes, and then contracts, pushing it into the stomach.
Good chewing saturates food with a large amount of saliva, it becomes more liquid, which facilitates and accelerates the passage of the food bolus into the stomach, so food should be chewed as long as possible. Liquid food passes through the esophagus in 0.5-1.5 seconds, and solid food in 6-7 seconds.
At the lower end of the esophagus there is a muscle constrictor (sphincter), which prevents the backflow (reflux) of acidic stomach contents into the esophagus.
The wall of the esophagus consists of 4 membranes: connective tissue, muscle, submucosa and mucosa.
The mucous membrane of the esophagus is a longitudinal fold of stratified squamous non-keratinizing epithelium that provides protection from damage by solid foods.
The submucosa contains glands that secrete mucus, which improves the passage of the bolus. The muscular layer consists of 2 layers: internal (circular) and external (longitudinal), which allows food to move through the esophagus.
A feature of the movements of the esophageal muscles during swallowing is the inhibition of the peristaltic wave of the previous swallow by the next swallow, if the previous swallow did not pass into the stomach.
Frequent repeated swallows completely inhibit esophageal peristalsis and relax the lower esophageal sphincter.
Only slow sips and freeing the esophagus from the previous lump of food create conditions for normal peristalsis.
Anatomical characteristics
Topography of the stomach
The length of the stomach goes from top to bottom, from left to right, from back to front.
Skeletotopy of the stomach
- cardiac section, lat. pars cardiaca
- at the level of the VII rib on the left; - fundus of the stomach (vault), lat. fundus (fornix) ventricul
- at the level of the cartilage of the 5th rib on the left; - body of the stomach, lat. corpus ventriculi
- between the fundus of the stomach and the pyloric region, respectively; - pyloric section (pyloric), lat. pars pylorica
- at the level of the Th12-L1 vertebra on the right.
The fundus of the stomach is adjacent to the ribs, the pyloric region is adjacent to the spinal column.
Syntopy of the stomach
Adjacent to the stomach:
- in front - the left lobe of the liver;
- behind, on the left, above - the spleen;
- behind - the pancreas;
- below - loops of the small (jejunal) intestine.
Holotopy of the stomach
Covered with peritoneum on all sides (intraperitoneal), projected into the epigastrium (regio epigastrica).
Structure of the stomach
- anterior wall of the stomach, lat. paries anterior
- posterior wall of the stomach, lat. paries posterior
- lesser curvature of the stomach, lat. curvatura ventriculi minor
- greater curvature of the stomach, lat. curvatura ventriculi major
Catarrhal pharyngitis
This form is different in that it appears at the very beginning of the disease. Catarrhal pharyngitis is the mildest stage. So
same, as in other forms, it is characterized by a sensation of a foreign body, as if snot is running down the back wall of the throat, tickling, itching and discomfort in the oral cavity. Sometimes it becomes difficult and painful to swallow. This symptomatology provokes frequent expectoration, as well as coughing. In this case, catarrhal pharyngitis is always accompanied by redness of the back of the throat. The cough in the morning can be so strong that there are attacks of vomiting. If adequate therapeutic treatment is not started in time, pharyngitis develops into a hypertrophic form.
Complications from this disease can spread throughout the body. Moreover, they quite often arise both due to lack of treatment and after illiterate use of medications. This is why it is so important to be treated under the supervision of a doctor.
Histological characteristics
Histologically, only 3 sections of the stomach are distinguished, since the mucous membrane of the fundus and body of the stomach have a similar structure and are considered as a single whole.
The wall of the stomach is formed by four membranes: mucous, submucosal, muscular and serous.
Mucous membrane
The relief of the mucous membrane (MS) of the stomach is characterized by longitudinal folds, fields, and dimples. It consists of three layers: epithelial, lamina propria and muscular lamina.
Epithelium
Single-layer highly prismatic (columnar) glandular enterodermal type, lining the gastric pits, the same in all parts of the stomach. All its cells secrete a special mucous secretion onto the surface of the CO, covering the CO with a continuous layer 0.5 mm thick. Bicarbonate, diffusing into mucus, neutralizes hydrochloric acid. For the secretion of enzymes and hydrochloric acid into the lumen of the stomach, temporary channels are formed in the mucus layer. Mucus forms a protective barrier that prevents mechanical damage to CO and its digestion by gastric juice. This barrier is damaged by alcohol and aspirin.
The integumentary epithelium is completely renewed within 1-3 days.
Own record
It is formed by loose fibrous unformed connective tissue with a large number of blood and lymphatic vessels, contains diffuse accumulations of lymphoid tissue and individual lymph nodes. In the form of thin layers it passes between the glands of the stomach, which occupy the main part of this layer.
Stomach glands
The number of glands is about 15 million - simple, tubular, branched and unbranched (in the fundus of the stomach; divided into cardiac, proper (fundic) and pyloric.
- cardiac
- tubular, with highly branched end sections, often having a wide lumen. They are located in the cardiac part of the stomach, similar to the cardiac glands of the esophagus. They contain mucous cells (with a light LC, a flattened nucleus, lying basally), which produce mucoid secretion, bicarbonates and chlorides of potassium and sodium. There are also separate chief, parietal and endocrine cells (see below). - own (fundic) glands
are unbranched, located in the body and fundus of the stomach and numerically predominate over other types of glands.
In groups of 3-7 they flow into small gastric pits. They have a narrowed neck, an elongated body and a bottom. They consist of 4 types of cells: main, parietal (lining), cervical, accessory mucous and endocrine. chief cells
are most numerous in the area of the body and bottom of the gland. They have a pyramidal or cylindrical shape and a large core located basally. The CP is basophilic, granular, in the basal part of the cell and around the nucleus it contains a lot of grEPS, a well-developed CG, in which large secretory zymogenic granules are formed (containing pepsinogen and other proenzymes), accumulating in the apical part of the cell and released into the lumen of the gland. In the lumen of the stomach, pepsinogen is converted into active pepsin under the influence of hydrochloric acid. - parietal (parietal) cells
- predominate in the area of the gland body. Larger than the main ones. They have a rounded shape with a narrow apex facing the lumen of the gland, with which they protrude between the main cells, located outward from them. The nucleus lies at the center of the cell. In the oxyphilic CP there are many large MTX with developed cristae and special intracellular secretory tubules in the form of narrow slits into which numerous myrrh-hairs face. - Along the periphery of the tubules there is a tubulovesicular complex - a system of membrane vesicles and tubules (a reserve of the membrane containing ion pumps), which merge with the tubules during active secretion. Parietal cells through the apical pole secrete hydrogen and chlorine ions, which, taken together, represent hydrochloric acid, creating an acidic (pH<2) environment in the lumen of the stomach. The latter provides: destruction of proteins;
- the conversion of pepsinogen to pepsin and the optimum pH for the activity of the latter;
- inhibition of the growth of pathogenic microorganisms.
Through the basal plasmalemma, the parietal cell secretes bicarbonate ions, which are carried by capillaries of the lamina propria to the basal surface of the integumentary cells, transporting them to the mucus, where they neutralize hydrochloric acid. Parietal cells also synthesize and secrete an antianemic factor, which, having formed a complex with vitamin B12, is absorbed in the ileum and is necessary for normal hematopoiesis. If this factor is insufficient (as a result of autoimmune damage to parietal cells or after removal of the stomach), pernicious anemia develops. Parietal cell secretion is stimulated by histamine, gastrin and acetylcholine.
- mucous cervical cells
are few in number and located in the cervix. Small sizes. The cytoplasm is weakly basophilic, granular, contains a moderately developed grEPS and a large supranuclear CG, from which large mucous granules are separated, accumulating at the apical pole. These cells often divide and are considered cambial elements of the epithelium of the glands and the integumentary epithelium of the stomach, where they, upon differentiation, migrate. Cell renewal in the glands occurs much more slowly than in the surface epithelium. The mucus produced by the cervical cells may protect them from damage. - accessory mucous cells
- located in the body of their own glands and have a compacted nucleus in the basal part of the cells. In the apical part of these cells, many round and oval granules and a small amount of Mx and KG were found. - endocrine cells
- located in the bottom of the glands. Light, varied in shape (triangular, oval or polygonal). The apical pole contains the nucleus and does not always reach the lumen of the gland. In the basal pole there are dense secretory granules released into the blood. The granules are covered with a membrane, colored with silver and chromium salts and contain peptide hormones and amines. They belong to the DES and APUD system, and are divided into EC, ECL and G cells. They produce hormones that affect secretory activity and motility of the digestive tract:
- D: somatostatin (body, pyloric region) - inhibits the secretion of GEP cells and gastric glands;
- EC: serotonin, motilin, substance P (body, pyloric region) - enhances intestinal motility;
- ECL: histamine (body) - increases the secretion of hydrochloric acid by the stomach;
- pyloric glands
are tubular, with highly branched and convoluted terminal sections. Located in the pyloric region. They flow into very deep gastric pits. They are formed by mucous cells, the secretion of which protects CO from acidic gastric juice. Most glands do not contain parietal cells. Mainly represented by endocrine cells (see above):
- D: somatostatin (body, pyloric region) - inhibits the secretion of GEP cells and gastric glands;
- EC: serotonin, motilin, substance P (body, pyloric region) - enhances intestinal motility;
- G: gastrin (pyloric region) - increases the secretion of hydrochloric acid and pepsinogen by the stomach;
- L: enteroglucagon (pyloric) - stimulates glycogenolysis in the liver.
Muscular plate
The muscular plate CO is formed by 3 layers of smooth muscle cells (inner and outer circular and middle longitudinal). From it, thin bundles of smooth muscle cells are directed into the spaces between the glands.
Submucosa
The RVNST is formed with many elastic fibers, in which large vessels and a submucosal nerve plexus are located. Participates in the formation of gastric folds.
Muscularis
It is formed by three thick layers of smooth muscle tissue: internal oblique, middle circular (most developed in the area of the pylorus, forms the sphincter) and external longitudinal. Between the muscle layers there are layers of loose fibrous connective tissue and elements of the intermuscular nerve plexus.
Serosa
Formed by a layer of mesothelium and underlying connective tissue.
What is the purpose of gastric histology?
https://www.youtube.com/watch?v=ytcopyrighten-GB
One of the organs of the digestive tract in which neoplasms often develop is the stomach. Histology should be performed if there is any change in the mucous membrane. The following diseases are considered indications for this study:
- Atrophic gastritis. This pathology is characterized by depletion of the cellular composition of the mucous membrane, inflammatory phenomena, and decreased secretion of hydrochloric acid.
- Rare forms of gastritis. These include lymphocytic, eosinophilic and granulomatous inflammation.
- Chronic peptic ulcer of the stomach and duodenum.
- Development of “small signs” according to Savitsky. These include general weakness, decreased appetite and performance, weight loss, and a feeling of abdominal discomfort.
- Detection of stomach polyps and other benign neoplasms.
- A sudden change in the clinical picture of a long-standing peptic ulcer. These include a decrease in the intensity of pain and the development of an aversion to meat food.
The listed pathologies refer to precancerous diseases. This does not mean that the patient has a malignant tumor and its location is the stomach. Histology helps determine exactly what changes are observed in the tissues of the organ. To prevent the development of malignant degeneration, it is worth conducting research as early as possible and taking action.
Physiology
The glands of the gastric mucosa secrete gastric juice containing the digestive enzymes pepsin, chymosin and lipase, as well as hydrochloric acid and other substances. Gastric juice breaks down proteins and partially fats, and has a bactericidal effect.
Main article: Gastric acidity
Due to the muscular layer, the stomach mixes food and gastric juice, forming chyme - a liquid pulp, which is removed in separate portions from the stomach through the pyloric canal. Depending on the consistency of the incoming food, it lingers in the stomach from 20 minutes (fruit juices, as well as vegetable juices and broths) to 6 hours (pork).
In addition, the stomach wall absorbs carbohydrates, ethanol, water and some salts.
Histology of the gastric mucosa
The mucous membrane of the digestive system is very thin. Its thickness does not exceed three millimeters, but this does not prevent it from being very, very durable and reliably protecting the body from pathogenic bacteria and toxins. Everything is thanks to a structure of three levels: the mucus layer, the epithelial and submucosal layers.
Mucus production is the first level of defense. It is produced by so-called goblet cells. Mucus envelops the food bolus and prevents it from injuring the delicate walls of the gastrointestinal tract. In case of damage, mucus fills the wound and thus speeds up healing.
Next comes a layer of epithelial cells. They are tightly adjacent to each other, which does not allow dangerous microorganisms to penetrate deep into the body and harm human health. Remember the pictures in which ancient warriors become shield to shield, create a wall and do not allow the enemy to pass? This is very similar to how epithelial cells work. To ensure maximum protection, they are held together by special proteins and form tight contacts.
True, this does not mean that the barrier is completely impassable. The “smart” mucous membrane filters which microbes can be passed through, and for which the “border is locked.” In tight junctions, channels can open that allow strictly defined components to pass through. Due to this, normal metabolism is maintained, and potentially dangerous compounds and bacteria remain “overboard”.
The mucous membrane is a reliable component of the gastrointestinal tract. If it were not so, a person would be endlessly ill and suffer from digestive problems. But the mucous membrane is not made of iron and can “crack” if the aggression factors are too powerful. What can damage the mucous membrane? No matter how trivial it may sound, these are unhealthy diets, alcohol, smoking, medications, stress, and inflammatory processes in the body. Age and heredity play a role.
The algorithm for restoring damaged mucous membranes is quite simple. First, the doctor determines the cause of the leaky gut. This may be one factor or a combination. The patient needs to give up alcohol, quit smoking - temporarily or forever, you need to understand the specific situation. The second component of therapy is diet. You should eat fractionally, in small portions and with gentle food - Table No. 1 and Table No. 5 according to Pevzner are suitable.
Literature
- Prives M. G., Lysenkov N. K.
Human anatomy. — 11th revised and expanded. - Hippocrates. — 704 p. — 5000 copies. — ISBN 5-8232-0192-3. - Afanasyev Yu.I., Yurina N.A.
Histology, cytology and embryology. — 5th revised and expanded. - M.: Medicine, 2002. - 744 p. — 10,000 copies. — ISBN 5-225-04523-5.
- Bykov V.L.
Private human histology. (Short overview course). Textbook. - St. Petersburg: SOTIS, 1999. - 304 p. — ISBN 5-85503-116-0 - Sapin M. R., Bilich G. L.
Human anatomy: textbook in 3 volumes - M.: GEOTAR-Media, 2008. - Volume 2. - 496 pp.: ill. ISBN 978-5-9704-0602-1 (vol. 2)
Links
- Stomach, anatomy // Encyclopedic Dictionary of Brockhaus and Efron: in 86 volumes (82 volumes and 4 additional). - St. Petersburg, 1890-1907.
- Stomach, physiology // Encyclopedic Dictionary of Brockhaus and Efron: in 86 volumes (82 volumes and 4 additional). - St. Petersburg, 1890-1907.
| Stomach | Pylorus |
| Small intestine | Duodenum · Major duodenal papilla · Sphincter of Oddi · Lesser duodenal papilla · Jejunum · Ileum · Ileocecal valve |
| Colon | Cecum · Appendix · Boosie's sphincter · Colon · Ascending colon · Transverse colon · Cannon-Boehm sphincter · Cannon's sphincter · Descending colon · Bally's sphincter · Sigmoid · Rectum · Rectal ampulla · Anal canal |
| Anus | Internal anal sphincter External anal sphincter |
| Large digestive glands | Pancreas Duct of Wirsung Duct of Santorini Liver Gallbladder Common bile duct |
An excerpt characterizing the human stomach
Katerina Petrovna really began to play waltzes and ecosaises, and dances began, in which Nikolai even more captivated the entire provincial society with his dexterity. He surprised even everyone with his special, cheeky style of dancing. Nikolai himself was somewhat surprised by his manner of dancing that evening. He had never danced like that in Moscow and would even have considered such an overly cheeky manner of dancing indecent and mauvais genre [bad taste]; but here he felt the need to surprise them all with something unusual, something that they should have accepted as ordinary in the capitals, but still unknown to them in the provinces. Throughout the evening, Nikolai paid most of his attention to the blue-eyed, plump and pretty blonde, the wife of one of the provincial officials. With that naive conviction of cheerful young people that other people's wives were created for them, Rostov did not leave this lady and treated her husband in a friendly, somewhat conspiratorial manner, as if they, although they did not say it, knew how nicely they would get together - then there is Nikolai and this husband’s wife. The husband, however, did not seem to share this conviction and tried to treat Rostov gloomily. But Nikolai’s good-natured naivety was so boundless that sometimes the husband involuntarily succumbed to Nikolai’s cheerful mood of spirit. Towards the end of the evening, however, as the wife's face became more ruddy and livelier, her husband's face became sadder and paler, as if the share of animation was the same in both, and as it increased in the wife, it decreased in the husband . Nikolai, with a never-ending smile on his face, sat slightly bent in his chair, leaning close over the blonde and telling her mythological compliments. Briskly changing the position of his legs in tight leggings, spreading the smell of perfume from himself and admiring both his lady and himself, and the beautiful shapes of his legs under the tight kichkirs, Nikolai told the blonde that he wanted to kidnap a lady here in Voronezh. - Which one? - Lovely, divine. Her eyes (Nikolai looked at his interlocutor) are blue, her mouth is coral, whiteness... - he looked at her shoulders, - Diana's figure... The husband approached them and gloomily asked his wife what she was talking about. - A! Nikita Ivanovich,” said Nikolai, standing up politely. And, as if wanting Nikita Ivanovich to take part in his jokes, he began to tell him his intention to kidnap a certain blonde. The husband smiled gloomily, the wife cheerfully. The good governor's wife approached them with a disapproving look. “Anna Ignatievna wants to see you, Nicolas,” she said, pronouncing the words in such a voice: Anna Ignatievna, that it now became clear to Rostov that Anna Ignatievna is a very important lady. - Let's go, Nicholas. After all, you allowed me to call you that? - Oh yes, ma tante. Who is this? – Anna Ignatievna Malvintseva. She heard about you from her niece, how you saved her... Can you guess?.. – I never saved them there! - said Nikolai. - Her niece, Princess Bolkonskaya. She is here in Voronezh with her aunt. Wow! how he blushed! What, or?.. - And I didn’t think, completeness, ma tante. - Well, okay, okay. ABOUT! what are you like! The governor's wife led him to a tall and very fat old woman in a blue cape, who had just finished her card game with the most important persons in the city. This was Malvintseva, Princess Marya's maternal aunt, a rich childless widow who always lived in Voronezh. She stood paying for the cards when Rostov approached her. She narrowed her eyes sternly and importantly, looked at him and continued to scold the general who had won against her. “I’m very glad, my dear,” she said, holding out her hand to him. - You are welcome to me. After talking about Princess Marya and her late father, whom Malvintseva apparently did not love, and asking about what Nikolai knew about Prince Andrei, who also apparently did not enjoy her favors, the important old woman let him go, repeating the invitation to be with her. Nikolai promised and blushed again when he bowed to Malvintseva. At the mention of Princess Marya, Rostov experienced an incomprehensible feeling of shyness, even fear. Leaving Malvintseva, Rostov wanted to return to dancing, but the little governor’s wife put her plump hand on Nikolai’s sleeve and, saying that she needed to talk to him, led him to the sofa, from which those who were there came out immediately, so as not to disturb the governor’s wife. “You know, mon cher,” said the governor’s wife with a serious expression on her kind little face, “this is definitely the match for you; Do you want me to marry you? - Whom, ma tante? – Nikolai asked. - I'm wooing the princess. Katerina Petrovna says that Lily, but in my opinion, no, is a princess. Want? I'm sure your maman will thank you. Really, what a lovely girl! And she's not that bad at all. “Not at all,” Nikolai said, as if offended. “I, ma tante, as a soldier should, do not ask for anything and do not refuse anything,” Rostov said before he had time to think about what he was saying. - So remember: this is not a joke. - What a joke! “Yes, yes,” said the governor’s wife, as if speaking to herself. - But here’s what else, mon cher, entre autres. Vous etes trop assidu aupres de l'autre, la blonde. [My friend. You look after that blond girl too much.] The husband is pathetic, really... “Oh no, we are friends,” Nikolai said in the simplicity of his soul: it never occurred to him that such a fun pastime for him could be for him. no one is having fun. “What a stupid thing I said, however, to the governor’s wife! – Nikolai suddenly remembered during dinner. “She’ll definitely start wooing, and Sonya?..” And, saying goodbye to the governor’s wife, when she, smiling, told him once again: “Well, remember,” he took her aside: “But here’s the truth.” tell you, ma tante... - What, what, my friend; Let's go sit here. Nikolai suddenly felt the desire and need to tell all his innermost thoughts (those that he would not have told his mother, sister, friend) to this almost stranger. Nikolai later, when he recalled this impulse of unprovoked, inexplicable frankness, which, however, had very important consequences for him, it seemed (as it always seems to people) that he had found a stupid verse; and yet this outburst of frankness, together with other minor events, had enormous consequences for him and for the whole family. - That's it, ma tante. Maman has long wanted to marry me to a rich woman, but the thought alone disgusts me, marrying for money. “Oh yes, I understand,” said the governor’s wife. – But Princess Bolkonskaya, that’s another matter; first of all, I’ll tell you the truth, I really like her, she’s after my heart, and then, after I met her in this situation, it’s so strange, it often occurred to me that this was fate. Think especially: maman has been thinking about this for a long time, but I had never met her before, as it all happened: we didn’t meet. And at a time when Natasha was her brother’s fiancée, because then I would not have been able to think about marrying her. It’s necessary that I met her exactly when Natasha’s wedding was upset, and then that’s it... Yes, that’s what. I haven't told this to anyone and I won't tell it. And only to you. The governor's wife shook his elbow gratefully. – Do you know Sophie, cousin? I love her, I promised to marry her and I will marry her... Therefore, you see that this is out of the question,” Nikolai said awkwardly and blushing. - Mon cher, mon cher, how do you judge? But Sophie has nothing, and you yourself said that things are very bad for your dad. And your maman? This will kill her, for one. Then Sophie, if she is a girl with a heart, what kind of life will she have? The mother is in despair, things are upset... No, mon cher, you and Sophie must understand this. Nikolai was silent. He was pleased to hear these conclusions. “Still, ma tante, this can’t be,” he said with a sigh, after a short silence. “Will the princess still marry me?” and again, she is now in mourning. Is it possible to think about this? - Do you really think that I will marry you now? Il ya maniere et maniere, [There is a manner for everything.] - said the governor’s wife. “What a matchmaker you are, ma tante...” said Nicolas, kissing her plump hand. Arriving in Moscow after her meeting with Rostov, Princess Marya found there her nephew with his tutor and a letter from Prince Andrei, who prescribed them their route to Voronezh, to Aunt Malvintseva. Concerns about the move, worries about her brother, the arrangement of life in a new house, new faces, raising her nephew - all this drowned out in the soul of Princess Marya that feeling of temptation that tormented her during her illness and after the death of her father, and especially after meeting with Rostov. She was sad. The impression of the loss of her father, which was combined in her soul with the destruction of Russia, now, after a month that had passed since then in the conditions of a calm life, was felt more and more strongly by her. She was anxious: the thought of the dangers to which her brother, the only close person left with her, was exposed, tormented her incessantly. She was preoccupied with raising her nephew, for whom she felt constantly incapable; but in the depths of her soul there was an agreement with herself, resulting from the consciousness that she had suppressed the personal dreams and hopes that had arisen in herself, connected with the appearance of Rostov. When the next day after her evening, the governor’s wife came to Malvintseva and, having talked with her aunt about her plans (having made the reservation that, although under the current circumstances it is impossible to even think about formal matchmaking, it is still possible to bring the young people together, let them get to know each other ), and when, having received the approval of her aunt, the governor's wife under Princess Marya spoke about Rostov, praising him and telling how he blushed at the mention of the princess, Princess Marya experienced not a joyful, but a painful feeling: her inner agreement no longer existed, and again Desires, doubts, reproaches and hopes arose. In those two days that passed from the time of this news to the visit to Rostov, Princess Marya continually thought about how she should behave in relation to Rostov. Then she decided that she would not go into the living room when he arrived at his aunt’s, that in her deep mourning it was indecent for her to receive guests; then she thought it would be rude after what he had done for her; then it occurred to her that her aunt and the governor’s wife had some kind of plans for her and Rostov (their looks and words sometimes seemed to confirm this assumption); then she told herself that only she, with her depravity, could think this about them: they could not help but remember that in her position, when she had not yet taken off her plereza, such matchmaking would be insulting both to her and to the memory of her father. Assuming that she would come out to him, Princess Marya came up with the words that he would say to her and that she would say to him; and sometimes these words seemed to her undeservedly cold, sometimes they had too much meaning. Most of all, when meeting with him, she was afraid of embarrassment, which, she felt, should take possession of her and betray her as soon as she saw him. But when, on Sunday after mass, the footman reported in the living room that Count Rostov had arrived, the princess did not show embarrassment; only a slight blush appeared on her cheeks, and her eyes lit up with a new, radiant light. -Have you seen him, auntie? - Princess Marya said in a calm voice, not knowing how she could be so outwardly calm and natural. When Rostov entered the room, the princess lowered her head for a moment, as if giving time to the guest to greet his aunt, and then, at the very time Nikolai turned to her, she raised her head and met his gaze with sparkling eyes. With a movement full of dignity and grace, she stood up with a joyful smile, extended her thin, gentle hand to him and spoke in a voice in which for the first time new, feminine chest sounds were heard. M lle Bourienne, who was in the living room, looked at Princess Marya with bewildered surprise. The most skillful coquette, she herself could not have maneuvered better when meeting a person who needed to please. “Either black suits her so well, or she really has gotten so prettier and I didn’t notice. And most importantly – this tact and grace!” - thought m lle Bourienne. If Princess Marya had been able to think at that moment, she would have been even more surprised than M lle Bourienne at the change that had taken place in her. From the moment she saw this sweet, beloved face, some new force of life took possession of her and forced her, against her will, to speak and act. Her face, from the time Rostov entered, suddenly changed. How suddenly, with unexpected, striking beauty, that complex, skillful artistic work appears on the walls of the painted and carved lantern, which previously seemed rough, dark and meaningless, when the light is lit inside: so suddenly the face of Princess Marya was transformed. For the first time, all that pure spiritual inner work with which she had lived until now came out. All her inner work, dissatisfied with herself, her suffering, desire for good, humility, love, self-sacrifice - all this now shone in those radiant eyes, in her thin smile, in every feature of her tender face. Rostov saw all this as clearly as if he had known her all her life. He felt that the creature in front of him was completely different, better than all those he had met so far, and better, most importantly, than himself. The conversation was very simple and insignificant. They talked about the war, involuntarily, like everyone else, exaggerating their sadness about this event, they talked about the last meeting, and Nikolai tried to divert the conversation to another subject, they talked about the good governor’s wife, about the relatives of Nikolai and Princess Marya. Princess Marya did not talk about her brother, diverting the conversation to another subject as soon as her aunt spoke about Andrei. It was clear that she could talk about the misfortunes of Russia feignedly, but her brother was a subject too close to her heart, and she did not want and could not talk lightly about him. Nikolai noticed this, just as he, with an astute observation unusual for him, noticed all the shades of Princess Marya’s character, which all only confirmed his conviction that she was a very special and extraordinary creature. Nikolai, just like Princess Marya, blushed and was embarrassed when they told him about the princess and even when he thought about her, but in her presence he felt completely free and said not at all what he had prepared, but what instantly and always opportunely came to his mind.
Cardiac department
The cardiac part of the stomach is the initial section of the organ. Anatomically, it communicates with the esophagus through an opening that is limited by the cardia (esophageal lower sphincter). Hence, in fact, the name of the department.
The cardia (a kind of muscular valve) prevents the reflux of gastric juice into the cavity of the esophageal tube. And this is very important, since the mucous membranes of the esophagus are not protected from hydrochloric acid (the contents of gastric juice) by a special secretion. The cardiac section, like other parts of the stomach, is protected from acid (acid) by mucus produced by the glands of the organ.
So what about heartburn? It causes a burning sensation and pain in the upper part of the stomach - one of the symptoms of reverse reflux (reflux of gastric juice into the esophageal tube). However, you should not rely solely on it as part of self-diagnosis. The upper section is the point at which pain of various natures can converge. Unpleasant sensations, pain, heaviness in the upper part of the stomach are also consequences of damage to the esophagus, gallbladder, pancreas and other digestive organs.
Moreover, this is one of the symptoms of dangerous conditions and pathologies:
- Acute appendicitis (especially in the first hours).
- Splenic infarction.
- Atherosclerosis of large abdominal vessels.
- Pericarditis.
- Myocardial infarction.
- Intercostal neuralgia.
- Aortic aneurysm.
- Pleurisy.
- Pneumonia, etc.
The fact that the pain is associated specifically with the stomach can be indicated by its frequency and occurrence immediately after eating. In any case, this will be a reason for a visit to a gastroenterologist - a doctor whose specialization includes diseases of the gastrointestinal tract.
In addition, heaviness in the initial gastric region may also indicate not a disease, but a banal overeating. The organ, the size of which is not unlimited, begins to put pressure on its neighbors, “complaining” about being overfilled with food.