Gigantism
(
gigantismus
; Greek gigas, gigant[os] giant) is a clinical syndrome that develops as a result of hyperproduction of growth hormone and is characterized by excessive, relatively proportional (Fig. 1) or disproportionate growth.
Rice.
1. A giant boy, 13 years old (on the left is a teenager of the same age). Gigantism occurs in the ratio of 1-3 per 1000 people.
Gigantism can occur with pituitary adenomas and other endocrine diseases associated with dysfunction of the hypothalamic-pituitary system - acromegaly (see), hypogonadism (see), Klinefelter's syndrome (see Klinefelter syndrome), dyspituitarism in adolescence (see dispituitarism in adolescence) -youthful).
Rice. 2. Partial gigantism in a woman: the right leg is enlarged.
Partial gigantism, in which individual parts or half of the body increase (Fig. 2), is considered as a developmental anomaly; Infections and injuries can trigger its occurrence.
Clinical picture
Patients complain of headaches, general weakness, memory loss, changes in appearance, and blurred vision. The growth rate is accelerating. At the beginning of the disease, the growth of the skeleton is relatively proportional; later, facial features may become larger, flat bones may thicken, the lower jaw, the spaces between the teeth, and the size of the hand and foot may increase. The scalp thickens, the voice becomes low, and macroglossia develops. The muscles that are overdeveloped at the onset of the disease atrophy, and muscle weakness increases. The function of the thyroid gland, gonads, and adrenal glands is impaired, and diabetes mellitus may develop.
Complaints
- headache;
- weakness;
- numbness in the hands;
- with acromegaly - change in appearance (body proportions, size of hands, feet, ears, nose);
- dry mouth and thirst (the result of the counter-insulin action of growth hormone);
- joint pain;
- limitation and pain in movements;
- almost all women have irregular menstrual cycles;
- 30% of men develop sexual weakness.
Causes of gigantism
Gigantism and acromegaly are two age-related variations of the same pathological processes: hyperplasia and hyperfunction of pituitary cells that produce somatotropic hormone (growth hormone). Increased secretion of growth hormone can be observed with lesions of the pituitary gland as a result of tumors of the gland (pituitary adenoma), intoxication, neuroinfections (encephalitis, meningitis, meningoencephalitis), traumatic brain injury.
Main symptoms
Gigantism begins to appear during puberty from 9-10 to 14-15 years. In some cases, the first symptoms may appear as early as 5-6 years of age. The disease occurs more often in boys than in girls.
In addition to increased growth, parents should be wary if their children complain of headaches and dizziness, joint and bone pain. Weakness and fatigue, visual impairment are noted. The teenager’s memory declines and the ability to adequately respond to school workload deteriorates. Physical indicators may be accompanied by mental abnormalities and suppression of sexual functions: amenorrhea in girls, hypogonadism in boys.
If gigantism is not detected in a timely manner and there is no treatment, other hormonal disorders begin to appear - diabetes, an increase or decrease in thyroid function. Internal organs suffer - the heart, lungs, liver, which do not have time to respond to the rapid growth of the body. Due to low sensitivity to sex hormones, the ossification process is not completed. The patient continues to grow after puberty. Very high chances of becoming infertile.
Treatment
Surgical removal of the pituitary gland (hypophysectomy) in a young animal results in growth arrest. Injecting such animals with growth hormone restores their normal growth. The administration of growth hormone to young growing animals sharply stimulates growth and leads to gigantism (in the experiment, rats, dogs and other animals were obtained that had a gigantic body size compared to the control).
In addition to growth hormone, the growth of animals and humans is influenced by many other factors, both environmental and genetic (see Phenotype). It has been noticed that when growth hormone preparations are administered to young patients, after 3-6 years from the start of therapy, sensitivity to exogenous (injected from the outside) growth hormone sharply decreases (the result of the production of antibodies).
Gigantism symptoms
Gigantism is classified into infantile and acromegalic forms. There are also two stages of the disease, such as stable and progressive.
The clinical picture of gigantism consists of complaints from adolescents in the form of weakness, dizziness, almost constant headaches, poor memory, pain in the limbs and increased heartbeat. In girls, there is an excessive increase in height and size of the feet, the mammary glands develop poorly, and in boys there is hyposexuality. Girls who are over 190 cm in height, and boys who are over 200 cm in height are very attracted to those around them.
Sometimes, in the symptoms of gigantism, a rough appearance appears in the foreground along with the general infantilism of a person. In addition, macrogenitalism is sometimes observed in young men. Patients with gigantism have a body weight that corresponds to their height, and their limbs are somewhat elongated.
The psyche of many patients is characterized by a certain underdevelopment in the form of average abilities, childishness, a tendency to depression and persecution mania.
People with gigantism always outperform others physically. Somatic organs are large, but this is usually not noticeable with high growth. But the size of the heart does not keep up with the growth of the body, which is why dizziness and fainting occur.
Depending on the hypertrophy and hyperplasia of soft tissues, macroglossia, diastema and enlargement of the larynx are noted. All this leads to changes in voice timbre, i.e. it sounds from the depths, very low. The ears, lips and nose also enlarge, and the lower jaw moves forward (prognathism). As a result of sinusitis, the mouth is often in a half-open position, as a result of which characteristic folds appear on the face. The skin becomes warm, moist, oily, hyperpigmented, and sometimes polyps, sebaceous cysts, acanthosis and hypertrichosis appear. The size of the head and foot increases. Sometimes kyphoscoliosis is diagnosed.
The functions of the organs are largely preserved, but gigantism still leads not only to cosmetic problems, but also to metabolic ones. Such patients rarely develop euthyroid goiter, as well as autoimmune thyroiditis. Diffuse toxic goiter can be observed less frequently.
With gigantism, glucose perception is reduced, similar to latent and overt diabetes mellitus, with resistance to conventional methods of therapy, as well as to insulin therapy. But hyperglycemia does not suppress the secretion of growth hormone.
Almost 30% of young people have decreased potency and libido, and girls have irregular periods. In addition, all patients have hyperprolactinemia.
In cases that are difficult to treat, secondary hypogonadism develops.
Gigantism can cause complications, which are manifested by panhypopituitarism, the development of acromegaly, diabetes mellitus, sexual disorders, myocardial dystrophy, and increased blood pressure. In more severe forms, patients lose their vision. Somatotropinoma can develop into malignant adenocarcinoma of the pituitary gland.
Links
- Media files on Wikimedia Commons
- Giants, pathology of growth // Encyclopedic Dictionary of Brockhaus and Efron: in 86 volumes (82 volumes and 4 additional). - St. Petersburg, 1890-1907.
To improve this article it is desirable:
Please, after fixing the problem, remove it from the list of parameters. After eliminating all the shortcomings, this template can be deleted by any participant. |
Etiology and pathogenesis
Overproduction of somatotropic hormone (see) is often associated with hyperplasia of eosinophilic cells of the pituitary gland (see). The cause of this overproduction may also be infectious processes in the interstitial-pituitary region. Gigantism is considered an age-related variant of acromegaly. In young people with incomplete ossification of the epiphyseal cartilages, overproduction of growth hormone can lead to increased periosteal and epiphyseal growth. An excess of this hormone in adults enhances periosteal bone growth and leads to a disproportionate increase in individual parts of the skeleton. This point of view does not explain, however, the reasons for the development of acromegaly in adolescence and childhood (including in newborns). It has been suggested that peripheral tissues have different sensitivity to growth hormone.
Gigantism usually develops over a number of years. An increase in height manifests itself in the prepubertal and pubertal periods, at the age of 10-15 years. Over time, acromegaloid enlargement of facial features, thickening of flat bones, and relative lengthening of the limbs may occur.
Forecast
With timely diagnosis of the disease and treatment, a favorable outcome of the disease is observed. It is worth treating nasopharyngeal disease in the early stages, avoiding hard work, and excluding traumatic brain injuries. If laboratory readings change, drug treatment should be started and the process stabilized.
If the disease progresses and is not treated, the outcome is cachexia. Life expectancy will be 3-4 years. With a slow development of the disease, up to 10 years of life from the onset of the disease.
Rate this article:
Signs and symptoms
There are total lesions of the limbs and localized, proportional, with uniform hypertrophy of all tissues, and disproportionate. Between these forms various intermediate forms are observed.
The size of a hypertrophied limb or its individual segments varies: in some cases, the circumference of the limb increases 2-3 times, and the elongation exceeds 10-15 cm. The relief and shape of the limbs also vary significantly.
With true gigantism in children, the skin is normal or slightly pigmented. If the giant growth is based on a vascular tumor, vascular spots of various sizes and colors are usually located on the skin or dilated vessels are visible. In neurofibromatosis, the spots are coffee-colored. With amniotic edema, diffuse erythrocyanosis is noted. The consistency of the tissues varies - from normal to very soft or, conversely, to hard with individual nodes, as in neurofibromatosis. The function of large joints is not limited. There are usually no obvious changes in the nervous system, with the exception of neurofibromatosis.
Localized gigantism of individual fingers of the upper and lower extremities, in some cases accompanied by hypertrophy of the entire hand or foot, deserves special attention due to its great cosmetic and functional significance. Most often, fingers III and II are affected, then fingers I, IV and V. Simultaneously with macrodactyly, syndactyly, polydactyly or microdactyly are sometimes observed. Damage to the fingers can occur as true or false gigantism. In this case, individual fingers can reach enormous sizes, take a forced bent or straightened position, deviate to the sides and push apart or cover adjacent fingers. Their movements are sharply limited. Working ability, wearing shoes and walking are very difficult.
Radiologically, with true proportional gigantism, all bones are uniformly increased in length and width. The timing of ossification is accelerated or, conversely, slowed down.
False gigantism is based on an increase in size as a result of a congenital abnormality of the vasculature, for example, an aneurysm or angioma, lymphangioma or lymphhemangioma, Meige's familial trophic edema or limited hereditary Milroy's edema, Recklinghausen's neurofibromatosis or persistent lymphatic edema developing below the amniotic strangulation groove and scar. With false gigantism, unlike true gigantism, bone elongation is rarely observed. In some cases, the size of the limb begins to increase only some time after birth. Some patients experience jerky growth, sometimes slow, sometimes fast.
The X-ray picture of false gigantism depends on the disease underlying the hypertrophic growth of the limb. Thus, with diffuse lymphangioma, or elephantiasis, caused by impaired lymph circulation, the bones are not changed; with neurofibromatosis, dystrophic changes of varying degrees may occur; with amniotic malformations, a wide variety of changes are observed: from synostosis and the atypical shape of individual bones to the complete absence of some of them.
Classification of gigantism
Modern endocrinology identifies the following options for the development of gigantism:
- Acromegalic – gigantism with signs of acromegaly;
- splanchnomegaly or gigantism of internal organs - accompanied by an increase in the size and weight of internal organs;
- eunuchoid - gigantism in patients with hypogonadism (hypofunction or complete cessation of the functions of the gonads), manifested by disproportionately elongated limbs, open growth zones in the joints, and the absence of secondary sexual characteristics;
- true - characterized by a proportional increase in body size and the absence of deviations in physiological and mental functions;
- partial or partial - gigantism with enlargement of individual parts of the body;
- half - gigantism, accompanied by an increase in one half of the body;
- cerebral - gigantism caused by organic damage to the brain and accompanied by intellectual impairment.
Causes of acromegaly and gigantism
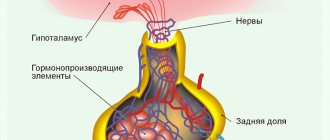
The pituitary gland is a small gland located at the base of the brain that produces certain hormones that are important for the functioning of other organs or systems of the body. Pituitary hormones are distributed throughout the body and are involved in a large number of processes, including the regulation of growth and reproductive functions. The causes of acromegaly in children lie in the excess production of growth hormones.
Under normal conditions, the pituitary gland receives input from another brain structure, the hypothalamus, located at the base of the brain. This signal from the hypothalamus regulates the production of hormones by the pituitary gland. For example, the hypothalamus produces a substance that directs the pituitary gland to begin the reaction of producing growth hormone. A signal from the hypothalamus should also stop this process if necessary.
In acromegaly, the pituitary gland continues to release growth hormones and ignores signals from the hypothalamus. At this time, the liver starts producing insulin-like growth factor, which is responsible for the growth of peripheral parts of the body. When the pituitary gland refuses to stop releasing growth hormone, insulin-like factor levels also peak and become abnormal. Bones, soft tissues, and organs throughout the body begin to enlarge, and the body changes its ability to process and use nutrients such as sugars and fats.
The most common cause of gigantism in children and acromegaly lies in the presence of a benign or malignant tumor in the pituitary gland, which is called a pituitary adenoma. In the case of pituitary adenoma, the tumor itself is a source of increased release of growth hormone in the blood. Because these tumors tend to grow quickly, they can press on nearby structures in the brain, causing headaches and blurred vision. When an adenoma grows, it can damage other pituitary tissues and disrupt the production of other hormones. These phenomena may be responsible for changes in the menstrual cycle and abnormal production of breast milk in women or lead to delayed development of reproductive organs. In rare cases, acromegaly can be caused by an atypical site of growth hormone production, leading to an abnormal increase in its amount. Some tumors in the pancreas, lungs, adrenal glands, thyroid gland and intestines can lead to overproduction of this substance.
Treatment of gigantism
The principles of treatment of gigantism are similar to the treatment of acromegaly. To normalize the level of growth hormone in gigantism, somatostatin analogues are used, and sex hormones are used to more quickly close bone growth zones. The etiological treatment of gigantism in pituitary adenomas involves the use of radiation therapy or their surgical removal in combination with drug support with dopamine agonists.
With the eunuchoid type of gigantism, treatment is aimed at eliminating sexual infantilism, accelerating skeletal ossification and stopping its further growth. Treatment for partial gigantism includes orthopedic correction through plastic surgery. The combined treatment of gigantism used by endocrinologists combines hormonal and radiation therapy and allows achieving positive results in a significant number of patients.
Diagnosis of gigantism
The diagnosis of gigantism is established on the basis of an external examination of the patient, the results of laboratory, radiological, neurological and ophthalmological studies. With gigantism, a high level of growth hormone in the blood is determined in the laboratory.
To identify pituitary tumors, radiography of the skull, CT and MRI of the brain are performed. In the presence of a pituitary adenoma, an enlarged sella turcica (pituitary gland bed) is determined. X-rays of the hands show a discrepancy between bone and passport age. An ophthalmological examination of patients with gigantism reveals limited visual fields and congestion in the fundus.