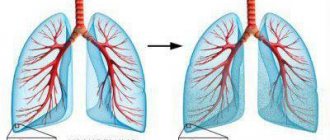
Pneumothorax is an accumulation of air in the pleural cavity - a normally slit-like space between the parietal (outer, lining the chest wall) and visceral (inner, covering the lung) layers of the pleura.
There are traumatic, spontaneous and iatrogenic pneumothorax. Traumatic pneumothorax occurs as a result of penetrating injury to the chest or damage to the lung (for example, fragments of broken ribs). Spontaneous (spontaneous) pneumothorax develops as a result of a sudden violation of the integrity of the visceral pleura, not associated with trauma or any therapeutic and diagnostic manipulation, leading to the entry of air from the lung into the pleural cavity. Iatrogenic pneumothorax is a complication of medical procedures.
Depending on the connection with the environment, closed, open and valve pneumothorax are distinguished. A closed pneumothorax is one in which the pleural cavity has no communication with the external environment and the amount of air entering it during injury does not change depending on respiratory movements.
With an open pneumothorax, there is a free connection between the pleural cavity and the external environment, as a result of which, during inhalation, air is additionally “sucked” into the pleural cavity, and during exhalation it comes out (“squeezed out”) in the same volume. Thus, with an open pneumothorax, there is no accumulation of air in the pleural cavity, and due to the unimpeded movement of air through the defect in the chest wall, the lung on the side of the wound collapses during inhalation, and during exhalation it increases in volume (expands), that is, the effect of paradoxical breathing occurs .
With valvular pneumothorax , in contrast to open pneumothorax, during exhalation the communication of the pleural cavity with the external environment is reduced or completely stopped due to the displacement of the tissues of the lung itself or the soft tissues of the chest, which can be compared to closing the valve. In this regard, during inhalation, a larger volume of air enters the pleural cavity than exits during exhalation. Consequently, during breathing there is a constant increase in the amount of air in the pleural cavity, which leads to progressively increasing compression of the lung, displacement of the mediastinal organs to the opposite (healthy) side, which disrupts their function, primarily squeezing large vessels, and with further progression leads to compression of the second lung on the “healthy” side.
If the air valve is located in the lung and the pleural cavity communicates with the external environment through the bronchial tree, then such a valve pneumothorax is called internal . If the valve is located in a wound of the chest wall, such a valve pneumothorax is called external . The internal and external valves cease to function independently when, at the height of maximum inspiration, the pressure in the pleural cavity reaches the pressure of the external environment, but at the same time the intrapleural pressure during exhalation significantly exceeds atmospheric pressure. The so-called tension pneumothorax , which is the outcome of the valve and is essentially a closed pneumothorax. However, tension pneumothorax differs from closed pneumothorax by much higher air pressure in the pleural cavity, significant displacement of the mediastinal organs, and compression of the lungs (complete on the affected side and partial on the opposite, “healthy” side).
Depending on the volume of air in the pleural cavity and the degree of collapse of the lung, limited (small), medium and large, or total pneumothorax is distinguished. With limited pneumothorax, the lung collapses by less than 1/3 of its volume, with an average - from 1/3 to 1/2 of the volume. With a large , or total, pneumothorax, the lung occupies less than half of the normal volume or is completely compressed with air.
Possible causes of pneumothorax
The causes of spontaneous pneumothorax can be (arranged in descending order of frequency):
1. Bullous lung disease. 2. Pathology of the respiratory tract (chronic obstructive pulmonary disease, cystic fibrosis, status asthmaticus). 3. Infectious diseases (Pneumocystis pneumonia, pulmonary tuberculosis). 4. Interstitial lung diseases (sarcoidosis, idiopathic pneumosclerosis, Wegener's granulomatosis, lymphangioleiomyomatosis, tuberous sclerosis). 5. Connective tissue diseases (rheumatoid arthritis, ankylosing spondylitis, polymyositis, dermatomyositis, scleroderma, Marfan syndrome). 6. Malignant neoplasms (sarcoma, lung cancer). 7. Thoracic endometriosis.
With spontaneous pneumothorax, the disease develops, as a rule, after physical exertion or severe straining, accompanied by an increase in intrapulmonary pressure.
Traumatic pneumothorax can occur with the following injuries to the chest:
1. Penetrating chest wounds (stab wounds, gunshot wounds). 2. Closed chest injury (damage from fragments of broken ribs, traumatic rupture of the lung).
Iatrogenic pneumothorax can develop as a complication of the following diagnostic and therapeutic procedures:
1. Puncture of the pleural cavity. 2. Catheterization of the central vein. 3. Pleural biopsy. 4. Transbronchial endoscopic lung biopsy. 5. Barotrauma during artificial ventilation.
In the past, the technique of therapeutic pneumothorax was used, in particular, in the treatment of cavernous pulmonary tuberculosis, when air was specially introduced into the pleural cavity to artificially ensure the collapse of the lung.
Classification
According to the etiological principle, primary and secondary are distinguished:
- Primary spontaneous pneumothorax is spoken of in the absence of evidence of clinically significant pulmonary pathology.
- The occurrence of secondary spontaneous pneumothorax occurs against the background of concomitant pulmonary diseases.
Depending on the degree of lung collapse, the following are distinguished:
- partial (small, medium). With a small spontaneous pneumothorax, the lung collapses by 1/3 of the original volume, with an average – by 1/2.
- total. With total pneumothorax, the lung collapses by more than half.
According to the degree of compensation of respiratory and circulatory functions
- The phase of stable compensation is for small and medium pneumothorax. There are no external manifestations of hemodynamic or respiratory disorders. In this case, VC and MVL can be reduced to 75%
- Unstable compensation phase – shortness of breath and tachycardia only during physical activity
- The phase of insufficient compensation (decompensation) - shortness of breath and tachycardia at rest, cyanosis, respiratory function are reduced by 2/3 or more from normal values.
Quite rare, but there are such forms of pneumothorax as:
- Menstrual. This form of the disease is closely related to thoracic endometriosis. More often, its development is observed in young girls in the first two days of the menstrual cycle. An important point that requires attention is that this form of the disease has a high risk of relapse. When diagnosing this pathological condition, it is often recommended to perform pleurodesis, which will help eliminate the risk of recurrence of pneumothorax.
- Neonatal. This form is rare and most often affects boys. May be associated with problems during lung expansion, respiratory distress syndrome, injury to lung tissue, and lung malformations.
The following are no exceptions:
- Diving underwater to great depths;
- Skydiving;
- Flying an airplane at high altitude.
All these reasons led to the formation of a pathological condition as a result of sudden changes in pressure, which act unevenly on different parts of the lungs.
Symptoms of pneumothorax
The main manifestations of pneumothorax are caused by the sudden appearance and gradual accumulation (with valve pneumothorax) of air in the pleural cavity and compression of the lung, as well as displacement of the mediastinal organs.
The onset of the disease is sudden: after a traumatic impact on the chest (with traumatic pneumothorax) or physical activity, straining (with spontaneous). Sharp stabbing or squeezing pains appear in the corresponding half of the chest, which are most often localized in the upper parts of the chest, radiating to the neck, shoulder or arm; sometimes the pain can spread mainly to the abdominal and lower back areas. At the same time, the patient experiences a peculiar feeling of tightness in the chest, as well as a subjective feeling of lack of air, which is accompanied by an increase in the frequency and depth of respiratory movements. With a large pneumothorax, the severity of shortness of breath is significant, it is accompanied by pallor or cyanosis (bluish coloration of the skin due to the accumulation of carbon dioxide in the blood), rapid heartbeat, and a feeling of fear. Trying to reduce pain and shortness of breath, the patient seeks to limit movements, takes a forced position of the body (half-sitting with an inclination towards the painful side or lying on the painful side).
With a significant volume of air in the pleural cavity, protrusion and limitation of mobility of the corresponding half of the chest can be determined, its lag in the act of breathing from the healthy one, which, on the contrary, breathes intensely, as well as smoothness of the intercostal spaces on the affected side. Often, especially with traumatic pneumothorax, subcutaneous emphysema is observed on the affected half of the chest - accumulation of air in the subcutaneous tissue of the chest wall, which can spread to other areas of the body with tension pneumothorax.
Kinds
Types of pneumothorax depending on the presence or absence of connection with the environment:
| pneumothorax | Symptoms in the lungs |
| open | If it develops, depressurization of the respiratory system occurs due to injury to the chest. Through the resulting hole, air gradually leaks into the pleural cavity during the act of breathing. Normally, the pressure in the chest is negative. If an open pneumothorax develops, it changes and this leads to the fact that the lung collapses and no longer performs its functions. Gas exchange in it stops, and oxygen does not enter the blood |
| closed | This type of medicine is considered the simplest. As a result of the progression of closed pneumothorax, a certain amount of gas accumulates in the pleural cavity, but its volume is stable, since the resulting defect closes itself. Air can leave the pleural cavity on its own. In this case, the lung, which was compressed due to its accumulation, is leveled out and the respiratory function is normalized; |
| tense | It is also called valvular pneumothorax in medical circles. This type of disease is the most dangerous and severe. A valve mechanism is formed in the chest, this leads to the fact that air enters the pleural cavity when inhaling, but does not leave it when exhaling. The pressure in the cavity will gradually increase, which will lead to displacement of the mediastinal organs, disruption of their functioning and to pleuropulmonary shock. When there is tension, air enters the pleural cavity through the wound. |
According to the presence of complications:
- Complicated (pleurisy, bleeding, mediastinal and subcutaneous emphysema).
- Uncomplicated.
By distribution:
- Unilateral.
- Bilateral.
In addition, pneumothorax can be:
- Parietal (the pleural cavity contains a small amount of gas/air, the lung is not fully expanded; as a rule, it is closed)
- Full (lung completely collapsed)
- Ensacculated (occurs when there are adhesions between the visceral and parietal pleura, limiting the area of pneumothorax; less dangerous, can be asymptomatic, but can also cause additional ruptures of lung tissue at the site of adhesions)
Survey
During percussion (percussion is tapping on individual parts of the body with subsequent analysis of the sound phenomena that arise during this), the doctor determines the “box” (loud and low, similar to the sound that occurs when beating on an empty box) nature of the percussion sound on the side of the pneumothorax, and when Auscultation of the lungs (auscultation is listening to sounds produced during the functioning of organs) reveals the absence or weakening of breathing on the side of the pneumothorax while breathing is preserved on the healthy side.
X-ray of a patient with a right-sided total pneumothorax (left on the X-ray). The arrow marks the border of the collapsed lung.
In making a diagnosis, an X-ray examination of the chest is of great importance, which determines free gas in the pleural cavity, a compressed lung, the degree of collapse of which depends on the size of the pneumothorax; with tension pneumothorax, the mediastinum shifts to the healthy side. Computed tomography of the chest allows not only to detect the presence of free gas in the pleural cavity (even with small limited pneumothorax, the diagnosis of which using conventional radiography is often quite difficult), but also to detect the possible cause of spontaneous pneumothorax (bullous disease, post-tuberculosis changes, interstitial lung diseases).
Computed tomogram of the chest of a patient with left-sided pneumothorax (on the tomogram - on the right). Free gas in the pleural cavity is indicated by an arrow.
What tests will you need to take if you suspect pneumothorax?
Laboratory examination for pneumothorax, as a rule, does not have independent diagnostic value.
Diagnostic methods
When examining the patient, the doctor notes the following:
- The characteristic position is sitting or semi-sitting. The patient is forced to take it to compensate for respiratory failure and reduce pain.
- The patient has shortness of breath, cyanosis, and breaks out in cold sweat. His chest expands, the intercostal spaces and supraclavicular spaces protrude.
- On the side where the lung is damaged, breathing movements are limited.
- Upon auscultation, it is noted that on the side with pathology, vesicular breathing and vocal tremor have weakened or are completely absent.
Today, one of the most accessible and most commonly used imaging methods for diagnosing spontaneous pneumothorax is radiography.
Instrumental studies
X-ray of the lungs reveals characteristic changes on the affected side:
- an area of clearing, devoid of a pulmonary pattern, located along the periphery of the pulmonary field and separated from the collapsed lung by a clear boundary. With a small pneumothorax, these changes may not be noticeable on an inspiratory radiograph. In this case, it is necessary to take an expiratory radiograph;
- displacement of the mediastinum towards the healthy lung;
- downward displacement of the diaphragm dome.
A pneumothorax of small volume is better identified in the later position - on the side of the pneumothorax there is a deepening of the costophrenic sinus and thickening of the contours of the lateral surface of the diaphragm.
The ECG reveals a deviation of the electrical axis of the heart to the right, an increase in the amplitude of the P wave in leads II, III, and a decrease in the amplitude of the T wave in the same leads.