Lung tissue is not supplied with many nerves. Therefore, if the pleura is involved in the pathological process, a person may not feel pain in the lungs (even in cases where the damage is extensive). Pain syndrome can develop due to irritation of the respiratory muscles and pleura when coughing. Changes are visible on x-ray and are detected during physical examination, especially when hypoxia and respiratory failure are present.
- Pneumonia
- Pulmonary edema
- Lung abscess
- Destructive damage to the lungs by staphylococci
- Gangrenous abscesses and gangrene
- Bronchiectasis
- Lung cysts
Lung damage is diagnosed by doctors of any specialty, and an accurate diagnosis must be made by a pulmonologist, therapist or thoracic surgeon. Most often, inflammatory lesions of the lungs are recorded, mainly pneumonia and bronchitis of various etiologies.
Pneumonia
Pneumonia is a diseased group of inflammations of the respiratory parts of the lungs with different etiologies (pathogens), pathogenesis and morphological characteristics. Inflammations are purulent, very rarely exudative. Other inflammatory processes are designated as pneumonitis, actinomycosis, tuberculosis, pneumoconiosis, echinococcosis, etc.
For example, with a closed chest injury, in 60 cases out of 100, infiltrative shadows are detected, which appear on the second or third day after the injury. This result of a bruise is called traumatic pneumonitis. On the 5-7th day, pneumonia may develop against the background of this process. “Pneumopathy” is a term used until the underlying disease that led to lung pathology is clarified. This includes syndromes:
- Hammena-Rici
- Wilson-Mikiti
- Leffler, etc.
Symptoms
Damage to the lungs and bronchi is manifested by coughing (with or without sputum, productive or unproductive), and attacks of suffocation. Also typical manifestations:
- hemoptysis
- shortness of breath with or without exertion
- increased breathing
- acrocyanosis
- cyanosis of the face, lips, tongue
- chills
- signs of intoxication
- fever
Diagnostics
Auscultatory methods normally record vesicular breathing without wheezing. There are 16-18 breaths per minute. With pathology in the bronchi, breathing is harsh, and buzzing or wheezing sounds are often heard. If lung tissue is involved in the process, doctors characterize breathing as weakened, large-, medium-, and fine-bubble rales or crepitus are heard.
Percussion diagnostic methods reveal a clear pulmonary sound. With emphysema, tympanitis is detected, with compaction due to infiltration, dullness of percussion sound, up to dullness with atelectasis, pneumofibrosis and cirrhosis or tumor.
In all cases of suspected lung damage, doctors prescribe a person an X-ray examination of the lungs (fluorography, or radiography). If pathologies are identified, a consultation with a therapist, pulmonologist, or thoracic surgeon follows. Additional tests may be ordered. Edema deserves special attention. In this condition, immediate assistance from a resuscitator is needed.
Diagnostic measures
If you notice symptoms that accompany bullous pulmonary disease, it is important to immediately contact a pulmonologist. The doctor examines the patient, listening to his breathing. If a disease is suspected, the patient is prescribed an x-ray or computed tomography. An analysis is also required to determine the gas composition of the blood.
In some cases, additional diagnostic methods may be needed: spirometry or peak flowmetry.
Pulmonary edema
This is a pathological lesion of the lungs, which is caused by profuse sweating of plasma into the interstitium and then into the alveoli of the lung. Most often, the cause is a cardiogenic factor in the development of left ventricular heart failure:
- valve prophets of the heart
- arterial hypertension
- coronary heart disease, etc.
Pulmonary edema is sometimes called cardiopulmonary syndrome. Lung damage can occur due to diseases and trauma of the lungs, when pulmonary hypertension and right ventricular failure develop. The cause of pulmonary edema may be portal hypertension, brain lesions, allergic conditions, excessive and rapid introduction of fluids into the bloodstream, intoxication, etc.
Symptoms of pulmonary edema are pronounced:
- forced semi-sitting position
- sharply rapid, labored, bubbling breathing, which can be heard even at a distance from the patient
- large amounts of frothy sputum, often pink in color
- rapidly increasing cyanosis of the skin
- acrocyanosis
- severe and painful suffocation
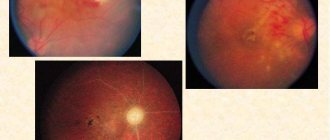
Hypoxic syndrome develops very quickly with the formation of hypoxic coma. A general clinical and physical examination may be sufficient for diagnosis. To clarify, two methods are used: radiography and ECG. The radiograph shows intense homogeneous darkening of the lung tissue in the central part and roots in the form of “butterfly wings”, or infiltrative-like darkening in the form of a “snow blizzard”. With pulmonary embolism, the darkening has a triangular shadow directed at an acute angle towards the root of the lung. With bronchial occlusion, pulmonary atelectasis is formed with homogeneous darkening of the lung tissue with a shift of the mediastinum towards the darkening, especially if the picture is taken during inspiration.
In most cases, lung lesions are managed by surgeons. Therefore, patients with documented pathology, which is described below, are hospitalized in surgical or thoracic pulmonology. We are talking, first of all, about suppurative lesions of the lungs.
What is pulmonology
The science that studies diseases of the lungs and respiratory tract is called pulmonology. The word itself comes from pulmo
– easy and
logos
– teaching. A little earlier, the science was called pneumology, but now this word is only a synonym for the name of the disease, and is not used in everyday life. Sometimes this section of medicine is also called respiratory or thoracic.
Today, pulmonology is the diagnosis, treatment and prevention of lung diseases. At the end of the 20th century, science became independent and due attention began to be paid to its study - the first pulmonology centers began to appear, new hospitals and departments in hospitals began to be built, and separate rooms began to be allocated for pulmonologists.
Modern pulmonology is:
- study of nonspecific lung diseases - diseases that, by their characteristics, do not belong to tuberculosis; allergies, pneumosclerosis
- studying pulmonary tuberculosis - another science deals with this - phthisiology, but recently scientists have come to the conclusion over and over again that tuberculosis is similar in its symptoms to other allergic, tumor or parasitic diseases of the lungs; hence the logical explanation for the reunification of two sciences into one
- study of occupational lung diseases - diseases caused by substances with which the patient comes into contact at his workplace
- study of lung tumors - the most dangerous of which is cancer
Lung abscess
This is a purulent-destructive lesion of the lungs with the formation of pathological cavities in it. The disease develops in most cases as a complication of pneumonia, which must be cured within 3 weeks. If the course lasts longer, a pulmonary abscess is suspected. It can develop only if 3 conditions are combined:
- the drainage function of the bronchi is impaired (walls, occlusion, etc.)
- specific or nonspecific pathogenic microflora invades the parenchyma
- blood flow in the lung tissue is disrupted, and necrotic processes develop
Types of abscesses:
- staphylococcal lung disease
- acute purulent abscesses
- widespread gangrene
- gangrenous abscesses
Also, abscesses can be multiple or single, the essence of which emerges from the name. There are two phases during:
- formation of a closed abscess;
- phase of the opened abscess (into the bronchus, into the pleural cavity, in both directions)
This lung damage is recorded mainly in males. An acute abscess occurs in phases. The patient may complain, until the ulcers are opened, of remitting or intermittent fever, weakness, profuse sweating, chills, persistent cough (mostly unproductive), which results in pain in the chest muscles. Breathing is rapid, mostly shortness of breath. Respiratory failure is likely.
Physical examination reveals dullness of percussion sound, lag of the affected side in the respiratory act, hard breathing, in some cases with a bronchial tinge. There are wheezing (dry or wet). X-ray can detect inflammatory infiltration of lung tissue without clear boundaries. A tomography method is relevant, which detects the presence of vacuum in the infiltration zone in case of lung abscess.
The bronchoscopic method detects a bronchus obstructed by fibrin, and after eliminating the occlusion in most cases, a large amount of purulent sputum immediately begins to flow. This phase can last from 10 to 12 days, unless a decision is made to open the abscess through a bronchoscope.
The transition to the second phase is sudden. The patient complains of a severe cough, which produces copious amounts of sputum. The patient coughs with his mouth full, while lying on the unaffected side, his torso hanging from the bed. The patient's condition becomes better, over time the fever decreases, breathing becomes more natural and uncomplicated. Percussion reveals tympanitis over the cavity, which intensifies when the patient opens his mouth and sticks out his tongue. The tympanic sound may become dull when the patient changes position (Weil's symptom).
An x-ray reveals an oval or round cavity containing fluid or air; a zone of perifocal inflammation is recorded, which decreases with treatment. If the course is favorable, the abscess will scar within 3-4 weeks. If it exists for more than 3 months, doctors talk about a chronic abscess, which can only be cured with surgery.
Content
The alveoli have a polygonal shape and are separated by interalveolar septa 2–8 µm thick. The interalveolar septa are represented by the walls of the alveoli, the elements of connective tissue located between them (elastic, collagen and reticular fibers) and a network of capillaries involved in gas exchange.
The total number of alveoli in both human lungs is 600-700 million. The diameter of one alveoli in a newborn child is on average 150 microns, in an adult - 280 microns, in old age it reaches 300-350 microns.
The inner layer of the alveolar wall is formed by squamous (respiratory) alveocytes (type 1 alveocytes) and large alveocytes (type 2 alveocytes), chemoreceptors (type 3 alveocytes), as well as macrophages. A significantly larger area is occupied by squamous (flat) cells. cells (97.5% of the inner surface of the alveoli) involved in gas exchange. Large alveocytes (granular, cuboidal, secretory cells), like respiratory alveocytes, are located on the basement membrane; these cells produce surfactant, a surface-active substance that lines the inside of the alveoli and prevents their collapse.
The aerohematic (air-blood) barrier between respiratory alveocytes and capillaries is formed by their basement membranes and is 0.5 microns. In some places, the basement membranes diverge, forming gaps filled with connective tissue elements. Each capillary participates in gas exchange with several alveoli.
Destructive damage to the lungs by staphylococci
It is recorded mainly in children, not adults. The course is rapid, hypoxia and intoxication syndrome appear. Hypoxic eclampsia often occurs. When coughing (persistent), an increasing amount of purulent sputum occurs. Auscultation reveals weakened breathing and cacophonous wheezing. X-ray shows extensive infiltration of lung tissue. On the second or third day after the onset of the disease, multiple cavities located in the cortical layer of the lung are recorded. The process very soon affects the pleura, pleurisy is formed. On the third day, the pleura generally breaks through, resulting in the formation of pyopneumothorax.
Forecast
COPD is a leading cause of disability and is the third leading cause of death in developed countries. Currently, chronic obstructive pulmonary disease is diagnosed in millions of people. And many more people may have this disease and not even know it.
COPD develops slowly. Symptoms often worsen over time and may limit your ability to carry out daily activities. Severe COPD can be almost completely incapacitating, preventing you from even basic activities such as walking, cooking or taking care of yourself.
Most cases of COPD are diagnosed in middle-aged or elderly people. The disease is not spread from person to person, so you cannot catch it from someone else.
COPD currently has no cure because doctors do not know how to reverse the damage to the airways and lungs. However, existing treatments and lifestyle changes can help you feel better, stay more active, and slow the progression of the disease.
Gangrenous abscesses and gangrene
They become a complication of pneumonia when putrefactive infection microorganisms, mainly Proteus, join. The patient's condition becomes even worse, hypoxia (lack of oxygen in the body) and intoxication phenomena are constantly increasing. A typical sign of this lung lesion is the early, abundant flow of foul-smelling sputum, which smells like foot wraps.
An X-ray of pulmonary gangrene shows darkening of the lung tissue. By the third, fourth or fifth day, several or one cavity is formed. The course in many cases becomes complicated over time by pulmonary hemorrhages, purulent pleurisy or sepsis.
Who is at risk for developing COPD
The main risk factor for developing COPD is smoking. Most people with COPD currently smoke or have smoked in the past. People with a family history of chronic obstructive pulmonary disease are usually more likely to develop this disease if they smoke.
Long-term exposure to other lung irritants is also a risk factor for developing COPD. Such irritants include:
- passive smoking
- air pollution
- chemical fumes
- dust in the environment
- house dust
Symptoms of chronic obstructive pulmonary disease usually begin to develop in people age 40 or older. It is quite rare for people under 40 to develop COPD. This can happen if a person has alpha-1 antitrypsin deficiency (an inherited disorder).
Bronchiectasis
This is a nonspecific lesion of the lungs and bronchi, in which they expand and purulent inflammation appears. The process is secondary, that is, bronchiectasis is acquired in 90-95 cases out of 100. They develop as a complication of chronic bronchitis in children and adolescents. The process primarily affects the lower lobe bronchi. Bronchiectasis can be unilateral or bilateral. Classification by form involves division into three groups:
- baggy
- cylindrical
- mixed
This lung damage does not develop immediately; exacerbations occur mainly in autumn and spring. But we are not talking about strict seasonal dependence. It is worth considering that cold and dampness are always provoking factors. The general condition remains unchanged for a long time. The only symptom during this period may be a persistent and frequent cough. It can be constant or intermittent. At first, sputum is released in small quantities, then the volume increases, reaching in some cases up to 1000 ml per day, especially in the morning. The temperature may periodically increase, reaching low-grade levels. During exacerbations, values can reach 38-39 degrees. With the development of bronchiectactic disease, pronounced symptoms develop due to increasing chronic hypoxia:
- puffiness of the face
- facial cyanosis
- acrocyanosis
- drumstick-shaped fingers
- watch glass shaped nails
- weight loss
- bloating of the chest (bulging ribs, widening of intercostal spaces)
- auxiliary muscles (the wings of the nose and the muscles of the shoulder girdle) are involved in the act of breathing.
The patient's breathing is characterized as rapid and heavy, and shortness of breath may be present. At the onset of the disease, chest x-ray and physical examination do not show the characteristic manifestations of bronchiectasis. With the obvious development of bronchiectasis, doctors record a boxy percussion sound, and in the lower sections - its dullness. In the upper sections, breathing is often harsh, and in the lower sections it is weakened. Dry or moist rales are detected.
On radiographs, especially tomograms, compaction of the roots and dense lower lobe bronchi are detected. Contrast bronchography shows a clear picture. A diagnostic method such as bronchoscopy is used. There are signs of chronic inflammation in them and the presence of a large amount of sputum, expansion of the lower lobe bronchi.
Due to chronic intoxication and lack of oxygen to the body, all organs and systems in the patient’s body are damaged to some extent. Therefore, surgical treatment is used in hospitals.
What are the lungs made of?
The human lungs are structured in a peculiar way - they completely lack muscle fibers, and a section reveals a spongy structure. The tissue of this organ consists of pyramid-shaped lobules, with their bases facing towards the surface.
The structure of the human lungs is quite complex, and is represented by three main components:
- Bronchi.
- Bronchioles.
- Acini.
This organ is saturated with 2 types of blood - venous and arterial. The leading one is the pulmonary artery, which gradually divides into smaller vessels .
In a human embryo, pulmonary structures begin to form at the 3rd week of pregnancy. After the fetus reaches 5 months, the process of formation of bronchioles and alveoli is completed.
By the time of birth, the lung tissue is fully formed, and the organ itself contains the required number of segments. After birth, the formation of alveoli continues until a person reaches 25 years of age.
“Skeleton” of the lungs – bronchi
The bronchi (translated from Greek as “breathing tubes”) are represented by hollow tubular branches of the trachea, connected directly to the lung tissue. Their main purpose is to conduct air - the bronchi are respiratory tracts through which oxygen-saturated air enters the lungs, and waste air flows saturated with carbon dioxide (CO2) are discharged back.
In the area of the 4th thoracic vertebra in men (5 in women), the trachea is divided into left and right bronchi, directed to the corresponding lungs. They have a special branching system that resembles the structure of a tree crown in appearance. That is why the bronchi are often called the “bronchial tree”.
The primary bronchi do not exceed 2 cm in diameter. Their walls consist of cartilaginous rings and smooth muscle fibers. This structural feature serves to support the respiratory organs and ensures the necessary expansion of the bronchial lumen. The bronchial walls are actively supplied with blood and penetrated by lymph nodes, which allows them to receive lymph from the lungs and participate in the purification of inhaled air.
Each bronchus is equipped with several membranes:
- external (connective tissue);
- fibromuscular;
- internal (covered with mucus).
A progressive reduction in the diameter of the bronchi leads to the disappearance of cartilage tissue and mucous membrane, their replacement by a thin layer of cubic epithelium.
Bronchial structures protect the body from the penetration of various microorganisms and keep the lung tissue in an intact state. When protective mechanisms are violated, they lose the ability to fully resist the effects of harmful factors, which leads to the occurrence of pathological processes (bronchitis).
Bronchioles
After penetration into the lung tissue of the main bronchus, it divides into bronchioles (the terminal branches of the “bronchial tree”). These branches are distinguished by the absence of cartilage and have a diameter of no more than 1 mm.
The walls of the bronchioles are based on ciliated epithelial cells and alveolocytes that do not contain smooth muscle cells, and the main purpose of these structures is to distribute air flow and maintain resistance to it. They also provide sanitization of the respiratory tract and remove rhinobronchial secretions.
From the trachea, air goes directly into the alveoli of the lungs - small bubbles located at the ends of the bronchioles. The diameter of these “balls” ranges from 200 to 500 microns. The alveolar structure looks much like grape bunches.
The pulmonary alveoli are equipped with very thin walls, lined from the inside with surfactant (a substance that prevents adhesion). These formations make up the respiratory surface of the lungs. The area of the latter is prone to constant fluctuations.
Acini
The acini are the smallest pulmonary unit. There are about 300,000 of them in total. The acini are the final point of division of the bronchial tree, and form lobules from which the segments and lobes of the entire lung are formed.
Lung cysts
This is a lung lesion in which intrapulmonary cavitary formations of various origins are formed. Cysts are divided into two types: true and false. True ones are formed as a result of a malformation of the small bronchi; in these cases, an epithelial lining is found. False ones are the result of inflammation or injury; there is no epithelial lining. Echinococcal cysts are isolated separately. Typical symptoms are not observed; they are most often discovered during medical examinations with fluorography, or when complications arise (rupture with the formation of spontaneous pneumothorax, bleeding or suppuration). Treatment is only operative (surgical). However, in some cases (rarely) with a single cyst, treatment may not be required.
Another classification of cysts:
- congenital
- acquired (caused by some disease)
Depending on the number of cavities, cysts are divided into single and multiple. The latter type is also known as polycystic lung disease. Depending on their location, cysts can be unilateral or bilateral (if both lungs are affected).
Causes of lung cysts:
- infectious-inflammatory process in the lung (the sputum in such cases is purulent, discharged “a mouthful”, 300-500 ml of sputum is released per day, gray-green in color; often a complication of pneumonia, mainly in alcoholics, because their liver is damaged, protein synthesis is inhibited, which limits the inflammatory process. If the cause is gangrene of the lung, the patient is unconscious, aspiration/inhalation of vomit is recorded, sputum can be 1-2 liters per day, it contains blood impurities.)
- lung tumors in the decay stage (this includes causes such as cancer)
- dystrophic disorders in the lungs (often occurs with pulmonary emphysema, when the connective tissue framework is too thin; this reason is typical for smokers who have been exposed to the bad habit for 10 years or more)
- lung malformations
Traditional methods of treatment
Those suffering from the bullous form of emphysema can use traditional methods of treatment as auxiliary means. Most often they resort to using potatoes. It is applied to the chest in boiled form, the juice from the tops of plants is drunk, and its vapors are inhaled.
The following recipes have also proven effective:
- Pour 300 ml of boiling water over 4 teaspoons of butterbur and leave for 1 hour. The infusion is taken twice a day, 2 teaspoons.
- Mix equal amounts of licorice and marshmallow root, anise, sage and pine packs. Pour in and strain after 3 hours.
- Pour 0.5 liters of boiling water over 100 g of buckwheat. Take 0.5 cups every 4 hours.
Althea for illness
Prevention of COPD
You can start taking some steps to prevent the development of COPD before it starts. If you are already suffering from this disease, you can take steps to prevent complications and slow the progression of the disease.
Preventing COPD before it starts
If you don't smoke, never try to start smoking, as smoking is the main cause of chronic obstructive pulmonary disease. If you already smoke, you need to completely quit this bad habit. If you smoke and want to quit but are unable to do so on your own, talk to your doctor about programs and tools that can help you quit smoking.
Also, try to avoid inhaling harmful substances that irritate the lungs, as exposure to them may contribute to the development of COPD. Passive smoking, air pollution, chemical fumes and dust can cause the development of this disease.
Preventing the development of complications and slowing the progression of COPD
If you are already showing the first signs of COPD, the most important step you can take is to quit smoking completely. This may help you prevent complications from developing and slow the progression of the disease. You should also avoid exposure to the lung irritants mentioned above.
Follow the COPD treatment plan your doctor has given you. This can help you breathe easier, stay more active, and avoid developing and keeping severe symptoms under control.
Talk to your doctor about whether you should get flu and pneumonia shots. These vaccines may reduce the risk of these diseases (not enough evidence - vaccines can be life-threatening), which are the main health risks for people with COPD.