Causes of polycystic kidney disease
The main causes of this pathology are a genetic factor. At the same time, cases of both recessive and dominant inheritance are known. It is worth noting that the latter inheritance occurs in families where both parents suffer from these diseases. In this case, the symptoms of polycystic disease are more pronounced and occur earlier. Along with hereditary forms of the disease, there are cases of the disease associated with the nephrotoxic effect of medications taken during pregnancy.
Classification
In humans, there are two main forms of polycystic kidney disease, differing in the type of inheritance: autosomal recessive polycystic kidney disease (typical of childhood) and autosomal dominant polycystic kidney disease (more often begins to manifest itself at the age of 30-50 years).[2]
Autosomal recessive polycystic kidney disease is associated with a mutation in the PKHD1 gene, which encodes the protein fibrocystin.[3]
Autosomal dominant polycystic kidney disease occurs in the human population with a frequency of 1/400 - 1/1000, being one of the most common genetic diseases. The total number of patients in the world is estimated at 10-12 million people. 85% of cases of autosomal dominant polycystic kidney disease are caused by a mutation in the PKD1 gene, located in the 16p13.3 region and encoding the polycystin-1 protein (in this case, the average age of development of end-stage renal failure is 54 years), 15% of cases are associated with a mutation of the PKD2 gene in the region 4q21 and encoding the protein polycystin-2 (the average age of development of end-stage renal failure is 74 years)[4][5].
Autosomal dominant polycystic kidney disease is inherited from parents in 90% of cases, while in about 10% of cases it is the result of spontaneous gene mutations.
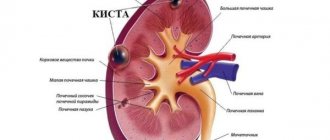
The cystic structures themselves are of 2 types:
- Closed capsules. These are closed cavities that have no connection with the urinary duct. This form of formation is more often detected in newborns with autosomal recessive polycystic kidney disease.
- Open. They are protrusions of the walls of the tubules that communicate with the pelvis. When such forms, more characteristic of autosomal dominant polycystic kidney disease, occur, the excretory function of the organ persists for a long time.[6]
In addition, cysts in the kidneys can also form in other diseases, but in this case their development is associated with mutations of other genes.
Stages of polycystic kidney disease
For convenience, the following stages are distinguished during the course of polycystic kidney disease:
Asymptomatic or preclinical. Its main characteristic is the absence of any changes at all in health, as well as in laboratory tests. This is the stage of complete compensation of kidney function and in fact the person is healthy. Making a diagnosis at this stage is associated with an ultrasound examination or other types of instrumental examination, in which kidneys with cysts present in them are detected.- Stage of laboratory changes. Some authors combine the first two stages into one. Nevertheless, at this stage, polycystic kidney disease can be suspected due to a slight decrease in their functionality when conducting laboratory stress tests. But since it is impossible to reliably diagnose polycystic disease based on these samples alone (an experienced doctor can only suspect it), then to verify or confirm it, instrumental examination methods are needed - the most common and safe, as well as informative - ultrasound.
Important! The above stages occur in “adult-type polycystic disease,” when the number of cysts is small and there is a significant percentage of healthy kidney tissue.
- Compensated clinical changes. These are mainly common infectious diseases of the kidneys and urinary tract - pyelonephritis. In addition, polycystic kidney disease is characterized by a predominance of general symptoms, such as headaches, decreased performance, and increased fatigue. Laboratory tests reveal signs of inflammation of the kidney tissue with a decrease in the functionality of the kidneys. Therapeutic treatment regimens can achieve significant improvement in a person’s condition.
- Decompensation of the disease. It is essentially classical and manifests itself as a combination of “kidney complaints” and general intoxication of the body. There is a constant exacerbation of inflammatory kidney diseases that cannot be treated with antibiotics. The emergence of persistent arterial hypertension with a crisis course and low effectiveness of antihypertensive drugs. Manifestations of intoxication in polycystic kidney disease at this stage include headache, constant nausea and frequent vomiting. Such patients suffer from insomnia, they are almost constantly in bed due to rapid fatigue, which is further increased due to severe anemia. Intensive treatment measures help cope with decompensation for a certain period of time.
- Terminal stage. At its core, it is renal failure and occurs in the absence of treatment with constant progression of the disease. This is especially true for “polycystic childhood type”, in children from parents with the same disease. The combination of severe heredity, rapid progression of the disease and adequate medical examination and care very quickly leads the patient to complete dependence on an intervention such as hemodialysis or an “artificial kidney”. The prognosis in some cases is unfavorable, and in others people on an “artificial kidney” live for many decades.
How does it manifest clinically?
With a disease such as polycystic kidney disease, the symptoms are as follows:
- There is pain in the area of the projection of the kidneys, varying in intensity, which often radiates to the side and intensifies with palpation. The pain is most often bilateral, and is caused by an increase in the size of the kidneys, stretching of the capsule, and compression of blood vessels and nerves.
- Organs increase in size, which can be confirmed by bimanual examination and ultrasound.
- Urolithiasis often occurs, blood appears in the urine, and is accompanied by symptoms of renal colic.
- Complicated by pyelonephritis, suppuration or rupture of the cyst, as well as hypertension.
- Heart rhythm disturbances appear, extrasystoles are detected. This is due to the fact that with polycystic disease the electrolyte composition of the blood changes and anemia develops.
- Renal failure develops with characteristic symptoms of constant dry mouth, itching, thirst, severe weakness and polyuria with a decrease in urine concentration. The patient has no appetite, and signs of exhaustion are increasing.
Examinations for suspected polycystic kidney disease
To establish a diagnosis of polycystic kidney disease and determine the type of disease, modern medicine uses a huge arsenal of informative methods and tools, including:
Study of parental heredity and genetic counseling.
- Carrying out ultrasound diagnostics (ultrasound) of the fetus several times during pregnancy, and the period starting from the 30th week is considered indicative.
- Carrying out ultrasound systemically for a newborn, as well as for a child aged 1 year. If necessary, control studies are carried out to evaluate the results over time.
- Laboratory diagnostics still plays a more significant role during the period of clinical manifestations to assess the functional capabilities of the kidneys.
- Instrumental methods such as X-ray contrast secretory urography (injection of a special substance into a vein and assessment of its excretion by the kidneys on a series of X-ray images), computed tomography, as well as more expensive MRI and PET are used to clearly visualize cysts when deciding on the possibility of surgery, as well as in preparation for surgery in order to select tactics and the scope of the planned operation.
Experimental treatments
Although there is no clinically tested effective treatment, all over the world there is an active search for drugs aimed at slowing the growth of cysts and inhibiting the development of renal failure specific to polycystic disease.
In clinical trials involving humans, drugs whose effect is associated with a decrease in the accumulation of cyclic adenosine monophosphate in cells (somatostatin analogues, vasopressin V2 receptor antagonists, mTOR inhibitors) are actively being studied.
There are also a number of drugs that have been studied only in laboratory animals. In particular, O. Yu. Beskrovnaya showed in laboratory mice the possibility of blocking the development of PBP by inhibiting cyclin-dependent kinases (that is, stopping the proliferation of the cyst epithelium)[5], as well as by inhibiting the synthesis of glycosylceramide[11].
Treatment of various forms and stages of polycystic kidney disease
Depending on the specific form of polycystic kidney disease, as well as the stage of development of the disease in a particular patient, certain optimal therapeutic measures are used.
Treatment of adult-type polycystic disease with unilateral kidney damage
The most favorable course and outcome is for polycystic disease of the “adult type” with unilateral kidney damage. In this clinical situation, the disease can be detected by chance during a general ultrasound examination and does not require any medication due to its compensation. The presence of inflammatory changes in the cyst requires general measures according to the severity of the manifestations.
Typically, for the treatment of such polycystic kidney disease, selected antibiotic therapy is prescribed in combination with anti-inflammatory drugs and mild diuretics. General strengthening drugs and vitamins are perfect. In combination with diet and lifestyle correction, such treatment can reliably avoid exacerbation of the disease.
Treatment of adult-type polycystic disease with bilateral kidney damage
Polycystic “adult type” with bilateral lesions and a small number of cysts on each kidney - on average from 22 to 50 cysts. Both the course and prognosis depend on the frequency of inflammatory complications and the rate of increase in cyst volume.
A wide range of medications are used for treatment. The most effective detoxification therapy is with anti-inflammatory drugs and antibiotics.
In some cases, an “artificial kidney” device is used to increase the effectiveness of treatment measures. General strengthening measures, vitamin therapy and maintaining a healthy lifestyle become dominant during the period of remission and are aimed at reducing the frequency and duration of periods of exacerbation of the disease.
Treatment of “childhood type” polycystic disease with multiple cysts on both kidneys
Polycystic disease of the “childhood type” with multiple cysts on both kidneys is the most difficult to treat. A significant number of cysts and small volumes of normally functioning renal tissue, the amount of which is steadily decreasing, over time lead to an early clinical manifestation in the form of decompensation of the disease, as well as pronounced manifestations that require the same measures that are adequate in effectiveness.
The main place in the treatment of this form of polycystic kidney disease is played by detoxification therapy and measures that support remission, which in this case is called “medical remission.” This emphasizes the dependence of a person’s condition on the constant use of certain drugs. For this form of the disease, the “artificial kidney” device plays a special role, which often becomes vital for patients.
What is an “artificial kidney”
For a simplified understanding, the “artificial kidney” device is a complex system of various types of filters that, through their operation, imitate the function of human kidneys. The device is integrated into the human circulatory system and purifies the blood plasma of various types of toxins and returns already purified blood to the body. The procedure requires frequent and constant repetition due to the accumulation of not only toxins, but also metabolic products of other tissues.
The need and effectiveness of surgical methods for treating polycystic kidney disease
In the treatment of polycystic kidney disease, various types of surgical interventions are used, which can be both radical and palliative:
- Radical removal (excision) of cysts is used for a small number of cysts, both on one and on both kidneys. In this case, a prerequisite for carrying out this type of intervention is a sufficiently high percentage of normally functioning renal tissue, which is confirmed before surgery using laboratory and instrumental examination methods. The results of such interventions are favorable.
- Palliative resection of individual cysts - this method of treating polycystic kidney disease is used mainly in the event of such a severe, but fortunately quite rare complication as suppuration of the contents of the cyst. This type of surgical intervention allows one to avoid the further development of purulent complications from the kidneys, while the course of the underlying disease - polycystic disease - is not particularly affected, since most often this kind of complications arises in severe cases of the disease in weakened patients with decreased immunity.
- Resection of a polycystic kidney. It is carried out in situations with a unilateral form of the disease, when one of the kidneys simply does not function due to the abundance of cysts. This makes it possible to achieve normalization of the patient’s condition due to the absence of exacerbations and to avoid the occurrence of purulent and other types of complications in the diseased kidney. It should be noted that pure kidney removal is used relatively rarely; most often it is a preparatory stage for another type of surgical intervention.
- Transplantation or transplantation of a healthy donor kidney. Performed in accordance with all the rules of transplantology, it can provide the body with a functional and anatomical functional kidney. Complete engraftment of the donor kidney guarantees the patient's cure. In the future, the person follows all the necessary recommendations to strengthen his general condition, and also undergoes courses of therapy from the transplantologist.
Prognosis and life expectancy
As a rule, with the described disease, the prognosis will be unfavorable due to possible complications, as well as the strong development of cysts not only in the kidneys, but also in other organs.
General prognoses depend on the condition of the patients, treatment measures, and prevention.
The prognosis is influenced by the course of polycystic disease; for example, if the problem is actively developing, then urgent measures must be taken, which makes it possible to eliminate serious consequences, complications and deaths.
With polycystic disease, death often occurs, especially when the problem develops in newborns.
Adults die as a result of complications, which include failure and stroke.
The overall outcome can be affected by a brain aneurysm and the presence of infectious infections in the body, since it is infections that aggravate the course and prognosis.
Recovery does not appear often in medical statistics, but there is a possibility of recovery.
With proper and high-quality therapy, the chances of recovery increase. Treatment is carried out using complex methods, taking into account the main symptoms of the disease and the presence of other pathological processes.
The patient’s life expectancy directly depends on the causes and many external factors. The course of polycystic kidney disease plays a huge role.
If a person’s health condition deteriorates due to infection of the body, then life expectancy decreases.
It is important to adhere to the basic treatment rules and the entire process, and strictly follow the doctors’ instructions.
Self-medication does not give results for this disease, in addition, it can affect life expectancy, not for the better.
By following the basic rules, you can extend the years of your life, as well as improve the quality of the allotted years.
This is due not only to the relief of unpleasant symptoms and general improvement of the condition, but also to stopping the development of the disease.
Treatment can only be carried out under the guidance of an experienced specialist, and medications are selected for each patient individually.
Polycystic kidney disease is not a death sentence!
In situations where you or your relatives have been given a preliminary diagnosis of polycystic kidney disease, do not despair. The main thing that needs to be done is to contact a urologist or nephrologist. Then undergo a full examination under the guidance of a medical specialist. He evaluates and interprets the data from the examination you are undergoing and gives you a full diagnosis. Advances in medicine at the present stage make it possible to achieve high-quality remissions and compensation for even severe forms of the disease, provided that the prescribed treatment is adequate and correct.
Remember! In any case, try not to evaluate the examination results yourself, and especially do not self-medicate, even relying on medical knowledge. This is fraught with progression of the disease and the occurrence of complications from other organs and systems. Contact specialists and stay healthy.
General practitioner, Sovinskaya Elena Nikolaevna.
16, total, today
( 186 votes, average: 4.55 out of 5)
Urate kidney stones
Trauma to the urethra (urethra) in men and women
Related Posts
Main symptoms
The clinical picture of polycystic kidney disease has different types of manifestations. Signs of pathology may differ depending on the stage and course of the problem.
If a person is in the compensation stage, then there will be almost no characteristic manifestations; after a while the patient develops the following sensations:
- Feeling of pressure in the lumbar region.
- Pain syndrome in the abdominal cavity.
- Disturbances in the outflow of urine appear.
Problems with urination are caused by stretching of the paired organ. Due to this, characteristic symptoms can be supplemented and are manifested by frequent headaches, rapid fatigue and the appearance of blood in the urine.
At the compensation stage, the main work of the kidneys is not disrupted, so the main functions associated with excretory capabilities proceed normally.
During the subcompensation stage, characteristic manifestations become stronger and more pronounced.
The main symptoms vary and each person may experience different symptoms.
The clinical picture of the pathology is caused by the insufficiency of the paired organ; the main sensations of patients are as follows:
- Intense thirst that is difficult to quench.
- Dry mouth.
- Attacks of nausea.
- Headaches that can progress to migraines.
- Increased blood pressure is a common symptom that persists for a long time.
In some cases, there may be polyuria or erythrocyturia; the rate of leukocytes in the blood increases.
If purulent inflammation is added to polycystic kidney disease, then the signs change, patients will have:
- Feverish state, chills.
- Signs of general intoxication.
- Development of kidney stones.
If there are external factors that negatively affect the condition of the kidneys, for example, mechanical damage to the walls, pregnancy, additional diseases, then the problem worsens, it develops and possible infection of an infectious nature.
High blood pressure over a long period, without the use of therapeutic measures, leads to heart failure and other organ disorders.
In this condition, the risk of stroke increases, and there may be a vascular aneurysm.
Diagnostics
If these symptoms of pathology occur, it is important to immediately consult a qualified nephrologist or urologist. If polycystic kidney disease appears in children, you should first visit a pediatrician.
During the initial examination, the doctor interviews the patient. Particular emphasis is placed on finding out the family history - whether the patient has close relatives with the same diagnosis. Next, the sore spots are probed and blood pressure is measured in both arms (in older people, measurements are also taken in a standing position). To confirm the diagnosis, laboratory and instrumental diagnostic techniques are used.
Laboratory:
- Analysis of urine;
- Reberg's test;
- Zimnitsky's test;
- clinical and biochemical blood test.
Instrumental:
- Ultrasound of the kidneys;
- Ultrasound of the abdominal organs;
- ECG;
- Kidney CT;
- MRI;
- renal angiography.