Treatment
Bronchial spasm and an attack of suffocation are not an independent disease, but a syndrome, that is, a complex of symptoms united by a single pathogenesis. When a condition arises, therapy is carried out in 2 directions at once:
1. Relief of bronchospasm. Drugs for relieving bronchospasm in children are selected based on age.
2. Elimination of the provoking factor. Diseases that provoke pathological contraction of smooth muscle fibers are treated, contact with possible allergens is excluded.
For chronic diseases that provoke bronchospasm, first aid medications are selected for the patient. Using prescribed medications, a person can prevent suffocation or stop an attack at an early stage.
Bronchospasmolytics
Medicines are needed for first aid for bronchospasm. Bronchospasmolytics from different groups are used.
List of bronchospasmodic drugs:
1. Adrenergic agonists (Ephedrine, Salbutamol, Isoprenaline). They influence adrenergic receptors, causing relaxation of smooth muscles.
2. M-anticholinergics (Berodual, Atropine sulfate, Berodual). They have only a local effect and do not enter the bloodstream. Used in the form of inhalations.
3. Phosphodiesterase inhibitors or xanthines (Theophylline, Theobromine). Reduce the amount of calcium inside cells, causing relaxation of smooth muscles. These medications are prescribed for bronchospasm in adults. Phosphodiesterase inhibitors are rarely used in children due to the fact that the drugs affect blood pressure and can cause tachycardia.
4. Corticosteroids (Prednisolone, Beclomethasone, Hydrocortisone). Used in the treatment of bronchial asthma, can be used to eliminate suffocation.
5. Mast cell membrane stabilizers (Cromolyn, Ketotifen). Suitable to prevent the appearance of signs of bronchospasm in adults and children. Block the entry of calcium into mast cells, preventing the release of histamine. These are drugs that prevent, but do not relieve bronchospasm, and are not suitable for eliminating the resulting suffocation.
Medicines that allow you to relieve bronchospasm in an adult or child at home are prescribed in the form of tablets, sprays or nebulizer solutions. During an attack, inhalations are more effective, allowing them to act directly on the receptors and tissues of the bronchial mucosa. The tablets act more slowly and do not help much during an attack.
Eufillin
The medicine, thanks to aminophylline, has a complex effect on the body:
· relaxes smooth muscle fibers;
· expands the lumens of the bronchi;
· improves the functioning of the respiratory center;
· reduces blood pressure by reducing vascular tone;
· eliminates the resulting suffocation.
Eufillin for bronchospasm is administered intravenously or intramuscularly to ensure rapid elimination of respiratory disorders. Tablets for bronchospasm containing aminophylline help worse.
Xanthine derivatives
A pharmacological group of drugs that has a symptomatic effect. Xanthine derivatives are used to relieve bronchospasm when it is necessary to quickly restore the patency of the bronchial tree and eliminate tissue hypoxia.
Medicines based on theophylline can quickly relieve bronchospasm. The substance is included in the following medications:
· Teopek;
· Eufillin;
· Retafil.
Medicines eliminate the resulting spasm and reduce pressure in the pulmonary circulation. Xanthines are recommended when suffocation is accompanied by pulmonary hypertension.
Sprays
Sprays are a convenient dosage form that allows you to spray small particles of active substances directly onto the mucous membrane of the bronchial tract. The spray helps with bronchospasm quickly, sometimes immediately after inhaling the therapeutic suspension.
What will help better depends on the sensitivity of the tissues to the active component of the aerosol and on the cause of bronchospasm.
The most effective drugs
If attacks recur regularly, then you need to have medicine with you that allows you to quickly restore normal breathing. A doctor will help you choose the most effective drug for bronchospasm after examining the patient and finding out the reasons that provoke bronchial spasm. To relax the walls of the bronchus and reduce swelling of the mucous membrane, the following can be used:
· bronchodilators (Salbutamol, Clenbuterol);
· sympathomimetic bronchodilators (Berotec, Berodual);
· drug-steroids (Pulmicort, Beclazon);
· medications based on cromoglycic acid that have an antihistamine effect (Nalkorm, Intal);
· anticholinergics (Atrovent, Spiriva).
Medicines for bronchospasm in adults, taken in sprays or in the form of inhalations using a nebulizer, begin to act almost immediately. If an hour after using bronchospasmolytics there is no improvement, the patient should be taken to the doctor immediately. How to treat bronchospasm will be decided by pulmonologists, taking into account the clinical picture of the attack.
Recommendations on what to do for bronchospasm in children are the same as for adults. It is important to use only medications prescribed by your doctor and follow the age-appropriate dosage. Exceeding the pediatric dose when trying to quickly stop an attack can provoke paradoxical bronchospasm.
What causes bronchospasms?
Bronchospasm can be caused by respiratory diseases such as asthma or bronchitis, as well as by medications or allergens. Common causes of bronchospasm:
bronchial asthma;
emphysema or chronic obstructive pulmonary disease (COPD);
Chronical bronchitis;
viruses, bacteria and fungal infections of the lungs;
air pollution or smoke;
environmental allergens such as pet dander, pollen, mold and dust;
some food additives and chemicals;
chemicals used in cleaning products and manufacturing
cold weather;
general anesthesia, mainly causing irritation of the respiratory tract;
exercises;
blood thinners, such as for high blood pressure and nonsteroidal anti-inflammatory drugs (NSAIDs);
antibiotics.
Scientists are still not sure why exercise can cause bronchospasm in some people. Traditionally, exercise-induced bronchospasm was considered a symptom of asthma, but new research has shown that this is not the case.
The researchers also found that bronchospasm is associated with several types of atopic rhinitis, a chronic condition that causes the formation of dry crusts in the nasal cavity and gradual thinning of the mucous membrane. Researchers are also still trying to determine whether e-cigarettes cause bronchospasms. Nicotine has been shown to stimulate the nerve in the lungs, causing bronchospasms. Scientists have found that e-cigarettes containing 12 mg/ml nicotine can cause bronchospasms in guinea pigs. Some chemicals found in medications can also cause bronchospasm, although this is rare.
Medicines to prevent bronchospasm
To prevent the development of an attack, drugs are selected taking into account the factor that provokes suffocation. Can be used:
1. Mucolytics (ACC, Bromhexine). Thins mucus and improves expectoration. Prevents obstruction.
2. Cromones (Ketotifen, Cromoglin). Prevents the release of the histamine enzyme from mast cells, reducing the risk of allergic suffocation.
3. Bronchodilators (Broncholitin, Salbutamol). The increase in bronchial lumen occurs due to relaxation of smooth muscle fibers.
The drugs are used in courses if latent bronchospasm is detected by spirometry or for the treatment of diseases accompanied by frequent attacks of breathlessness.
To prevent symptoms of bronchospasm and provide supportive treatment in children, the same medications are used as in adults.
Diagnostic methods to help identify bronchospasm:
Spirometry - the patient inhales and exhales several times with moderate to maximum force through a tube connected to a computer.
Pulse oximetry - a device that measures the amount of oxygen in the blood and is attached to the finger or ear.
Arterial blood gas analysis—determines the levels of oxygen and carbon dioxide in the blood.
Chest X-ray and computed tomography (CT) scan—X-rays of the chest and lungs can help rule out a lung infection.
To determine whether bronchospasm is a result of exercise, your doctor may recommend a hyperventilation test. During this test, a person inhales a mixture of oxygen and carbon dioxide to determine how lung function changes.
How to quickly relieve bronchospasm
The resulting syndrome must be eliminated immediately. Prolonged bronchospasm leads to hypoxia. To competently provide first aid, you need to know how to relieve bronchospasm in a child and an adult.
First aid at home to relieve an attack
If a person begins to choke for the first time, then it is necessary to call an ambulance. Before paramedics arrive, you should try to alleviate the patient’s condition.
First aid algorithm for symptoms of bronchospasm in adults and children:
1. Remove the provoking factor (if known).
2. Unbutton or remove tight clothing so that things do not interfere with free breathing
3. Plant. A comfortable position that allows you to feel less out of breath: sitting, slightly leaning forward and resting your hands on your knees.
Symptoms of bronchospastic syndrome
If a person suffers from chronic diseases of the respiratory system and has already had bronchospastic attacks, he can easily determine their approach.
Characteristic signs of this phenomenon:
- lack of air, chest congestion;
- characteristic “wheezing breath”;
- dry cough that does not stop;
- pallor, possible cyanosis (cyanosis) of the nasolabial triangle;
- when inhaling, the wings of the nose and neck muscles are involved;
- the person experiences panic and fear.
These symptoms must be stopped immediately, otherwise the patient may faint and even die, because the amount of air that enters his lungs is minimal.
Review of reviews on the use of Salbutamol
On forums dedicated to pulmonary diseases, you can find various reviews about the use of Salbutamol for bronchospasm. Positive characteristics are given due to the fact that the drug promotes:
· rapid restoration of bronchial patency;
· relief from shortness of breath.
Patients note that the compact aerosol can is convenient to carry and the product is inexpensive.
But the medicine also has disadvantages. These include:
· a large number of side effects;
· weak therapeutic effect;
· cannot be used frequently due to the risk of addiction.
Salbutamol is an inexpensive, effective bronchodilator, and many patients with a tendency to spastic bronchial obstruction evaluate the aerosol positively. But the drug is not suitable for everyone. Despite the fact that negative reactions from the inhaler occur infrequently, the drug should not be used to ease breathing without the prescription of a pulmonologist.
Causes
Please note that if you are extremely careful, you can prevent a dangerous condition. It is important to consider factors that can lead to bronchospasm:
- Food, medicinal, household allergens.
- Dust, various chemicals, smoke, and other irritants with a strong aroma.
- Smoke from cigarettes.
- Mechanical irritation of the respiratory tract.
- Negative effects of certain drugs.
- Intoxication of the body due to a bacterial or viral infection that has entered the bronchi.
- Severe poisoning by fungus and helminths.
- Incorrect use of inhalational anesthetics.
- Exacerbation of chronic obstructive bronchitis, asthma.
- Stressful situation.
- Meteor dependence.
People who have a hereditary predisposition, who often suffer from allergies and atopic dermatitis, are most prone to spasms in the bronchi.
Bronchospasm is especially dangerous for young children; they suffer from ARVI, and the reaction can be unpredictable. The condition is also typical for those who have to constantly work in a factory with an unfavorable environment.
Diagnostics
Diagnosis of total bronchospasm is not difficult, unlike partial bronchospasm, which may have scant symptoms. In addition to the cyanotic tint of the skin, as well as moderate arterial hypertension, during visual inspection during thoracotomy, patients experience insufficient collapse of the lungs during exhalation, as well as increased resistance to artificial inspiration. Stable respiratory acidosis during vigorous artificial ventilation indicates the presence of a latent form of partial bronchospasm.
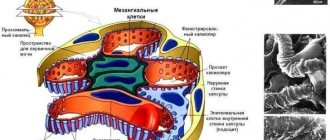
Studying the function of external respiration is of great importance for diagnosing bronchospasm. When carrying out hardware diagnostic methods, the minimum concentration or complete absence of carbon dioxide in the exhaled air is determined, while its concentration in the patient’s blood increases.
Endoscopic picture of bronchospasm, on the left – before, on the right – after the attack
Differential diagnosis is carried out with mechanical obstruction of the bronchi by a foreign body, kinking of the endotracheal tube, or atelectasis that developed acutely during anesthesia. It is often necessary to differentiate this pathological process from pulmonary edema; the latter may also be the terminal stage of bronchospasm.
At the initial stage of development of bronchospasm, the patient experiences bradycardia, arterial hypertension and low pulse pressure due to an increase in diastolic blood pressure, and a small amount of viscous glassy sputum is released. With pulmonary edema against the background of increased blood pressure, tachycardia develops, pulse pressure increases due to an increase in systolic blood pressure, then myocardial hypoxia occurs, followed by ventricular fibrillation and cardiac arrest. Patients with pulmonary edema produce frothy sputum mixed with blood.
– Clinical and biochemical blood tests.
– Sputum examinations.
– Capnography. This analysis allows the specialist to estimate the depth of breathing based on the amount of carbon dioxide in the air the patient inhales.
– Bronchophonography. Conducted using computer equipment. Allows you to study respiratory function even in infants. This method is used mainly with children.
– Pulse oximetry – allows you to determine the amount of oxygen in the blood, as well as the pulse rate, a change in which is observed during bronchospasm.
It is impossible to refuse the above diagnostic methods, because this is the only way the doctor will be able to understand the cause of the attack and do everything possible to ensure that it does not recur.
Primary diagnostic measures are usually carried out by emergency physicians and general practitioners in hospital emergency departments. Subsequently, the patient is examined by a pulmonologist; if necessary, allergists-immunologists and other specialists can be involved in the diagnostic search. The main research methods to detect bronchospasm are:
- Inspection. During examination, the color of the skin is assessed. With severe bronchoconstriction, the skin turns pale, the lips and terminal phalanges of the fingers appear blue. Noteworthy is the forced position of the patient's body and the participation of auxiliary muscles in breathing. In patients with bronchial obstruction due to chronic pulmonary pathology, distal hypertrophic osteoarthropathy is often observed.
- Percussion, auscultation. Percussion detects a box sound over the entire surface of the lungs. During auscultation, harsh breathing, dry wheezing on exhalation are heard, and less commonly, wheezing is heard at the height of inspiration. Tachypnea and increased heart rate are present. Severe life-threatening bronchospasm is characterized by the appearance of areas of “silent lung”, in the projection of which respiratory sounds are not heard.
- Pulse oximetry. During the study, a pulse oximeter measures arterial blood oxygen saturation and heart rate, and determines the degree of respiratory failure. Blood oxygenation less than 95% along with tachycardia is a sign of oxygen starvation. Hypoxia is considered critical when saturation is 90% or lower.
- Spirography. Study of the function of external respiration helps to differentiate obstructive disorders from restrictive ones. The presence of narrowing of the lumen of the respiratory tract is indicated by a decrease in FEV1 and Tiffno test. The use of a bronchodilation test allows us to detect the reversibility of bronchoconstriction.
- X-ray, CT scan of the lungs. They are auxiliary diagnostic methods. Used to determine the cause of secondary airway obstruction. X-rays and computed tomograms visualize pulmonary emphysema, detect radiopaque foreign bodies, tumors, enlarged lymph nodes, and signs of other pathologies of the respiratory tract.
In order to diagnose bronchospastic conditions in young children, bronchophonography is used. An increase in the content of carbon dioxide in exhaled air, determined using capnography, helps to detect bronchospasm in intubated patients. The function of external respiration can be most fully studied using body plethysmography.