Joint hypermobility, or unusual joint mobility, is quite common. Usually it disappears without a trace over the years. Sometimes the pathology remains and leads to serious complications.
Hypermobility syndrome is a condition in which some or all of a person's joints have an unusually large range of motion. Sometimes people call these loose joints or double joints.
Joint hypermobility syndrome is more common in children and young people than in older people. It is not known why some children with double ligament have sore muscles and others do not. Hypermobility syndrome is considered benign.
Causes
It is believed that a person with hypermobility may have more elastic tissues in their bodies, especially muscles and ligaments, than others. People vary greatly in this extensibility, and supermobility is probably simply the most elastic group of people in a broad but normal group.
No one knows why some children and adults with hypermobility develop complex symptoms while most do not, but it may be that these children and adults are the ones with the most elastic tissue.
Other factors may also contribute, including muscles that tend to be more relaxed at rest than average. There may also be natural changes in the shape of bone joints, so that some people's joints may go to greater extremes than other people's.
Increased joint mobility is inherited in specific genes passed on by parents to their children. This is what causes the pathology in newborns.
The cause of hypermobility is a change in a type of protein called collagen. As a result, connections may become longer than usual. In some cases, the causes of the pathology are associated with one of the types of Ehlers-Danlos syndrome. This syndrome affects collagen in the human body.
Rarely, joint hypermobility occurs as a result of a more serious condition such as:
- Osteogenesis defect is a condition that affects the bones.
- Marfan syndrome is a condition that affects the blood vessels, eyes and skeleton.
Notes[ | ]
- Disease ontology database (English) - 2020.
- Monarch Disease Ontology release 2018-06-29sonu - 2018-06-29 - 2018.
- V. B. Simonenko et al., Connective tissue dysplasia (Hereditary collagenopathies), “Clinical Medicine”, 2006, N 6, 62-68.
- JH Kirk, BM Ansell, EG Bywaters, The hypermobility syndrome, Ann. Rheum. Dis., 1967, 26, 425-427.
- A. G. Belenky, Hypermobility syndrome - a systemic non-inflammatory disease of connective tissue, Department of Rheumatology RMAPO, Moscow
- Hypermobility syndrome: clinical manifestations, differential diagnosis, approaches to therapy N. G. Pravdyuk, N. A. Shostak, Department of Faculty Therapy named after. A. I. Nesterova, Russian State Medical University, Moscow
- M. M. Bikbov, V. K. Surkova, K. Kh. Oganisyan.
Keratoconus as a manifestation of connective tissue dysplasia (Russian).
Ophthalmology
(March 31, 2015). Retrieved August 8, 2020. - Connective tissue dysplasia: main clinical syndromes, diagnosis, treatment. G. I. Nechaeva, V. M. Yakovlev, V. P. Konev, I. V. Druk, S. L. Morozov
- Attending physician
Symptoms
Benign joint hypermobility does not always cause difficulty or pain. Many people with hypermobility have no problems, and some, such as ballet dancers, gymnasts and musicians, actually benefit from their condition.
This pathology has several unpleasant symptoms:
- pain, often after physical work or exercise from overstrain of the joint capsule (the structure that surrounds the joint) and ligaments (the tough bands that bind two bones together),
- muscle pain (due to the fact that the muscles have to work harder with flexible joints),
- pain in the back and neck,
- tendency to bruise
- pain that increases during the day and decreases at night and after you have rested, fatigue (extreme fatigue),
- night pain in children.
Hypermobility syndrome can cause a wide range of symptoms, including symptoms that affect your digestive system and blood pressure.
Hypermobility tends to decrease with aging as we become naturally less flexible.
Hypermobility of the lumbar spine
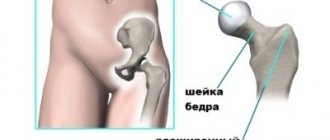
Segmental hypermobility of the spine in the lumbar region often develops in people engaged in heavy physical labor. Their diffuse nutrition of the cartilaginous tissues of the intervertebral discs is disrupted. They lose their normal height and do not hold the vertebral bodies in one position. Under any extreme load, for example, when lifting something heavy or suddenly straightening, there is a risk of the vertebral body slipping relative to its neighbor. This phenomenon is called retrolisthesis or antelisthesis (depending on whether the vertebral body is displaced anteriorly or posteriorly).
As the pathology develops, acute pain occurs, accompanied by muscle weakness in the lower extremities. Hypermobility of the lumbar spine must be diagnosed at an early stage and measures taken to compensate for it. If this is not done, there is a high probability of developing the following complications:
- displacement of the vertebral body and fixation in this position with pinching of the radicular nerve;
- stenosis of the spinal canal and the development of paresis and paralysis of the lower extremities, pelvic organs and abdominal cavity;
- insufficient function of the intestines, gall bladder, biliary tract, bladder, kidneys, etc.;
- deforming osteoarthritis of uncovertebral, facet and facet joints;
- destruction of the iliosacral joints of the bones;
- distortion of the pelvic bones;
- poor posture and curvature of the spinal column;
- destruction of intervertebral discs, etc.
If you suspect that you have hypermobility of the lumbar spine, we recommend that you make an appointment with a vertebrologist or neurologist as soon as possible. This is a serious pathology that can be treated conservatively only at an early stage.
Diagnosis of the syndrome
Hypermobility syndrome is diagnosed by examining the affected joints and noting that they easily fall outside the expected normal range.
Signs that doctors look for to confirm hyperplasticity include the following:
- Bend your thumbs onto your forearms,
- Elbows reaching beyond neutral to 10 degrees,
- Bend your fingers back 90 degrees
- Extend the knees vertically beyond normal to 10 degrees.
Hypermobility is difficult to measure because the extent of the condition varies from person to person. There is no blood test for hypermobility syndrome.
However, you can use a system called the Bayton Score to determine if you have joint hypermobility.
Beighton test
The Beighton assessment consists of nine tests, listed below. Each test is worth one point.
- Can you place your hands on the floor with your knees straight?
- Can you bend your left elbow back?
- Can you bend your right elbow back?
- Can you bend your left knee back?
- Can you bend your right knee back?
- Can you bend your left thumb back onto the front of your forearm?
- Can you bend your right thumb back on the front of your forearm?
- Can you bend your left little finger 90 degrees toward the back of your hand?
- Can you bend your right little finger 90 degrees toward the back of your hand?
Most people score less than two, but if you score four or more, you probably have hypermobility. The check is quite simple.
For an accurate diagnosis, you need to see an orthopedist.
Brighton criteria
If you also have symptoms such as joint pain, you may have joint hypermobility syndrome. Your doctor can diagnose this using the Brighton criteria. The Brighton criteria take into account your Beighton score and take into account other symptoms. There are major and minor Brighton criteria.
Brighton's main criteria:
- Having a Beighton score of 4 or more,
- Pain in four or more joints for more than three months.
Brighton secondary criteria:
- Beighton score 1-3,
- Joint pain (arthralgia) in 1-3 joints for more than three months,
- Back pain for more than three months
- Back condition in adolescents (spondylosis/spondylolysis/spondylolisthesis),
- More than three inflammatory conditions (eg, tendonitis),
- Tall, slender body with long fingers and toes,
- Dislocation of more than one joint or dislocation of the same joint at least twice,
- Thin elastic skin with paper scars,
- Drooping eyelids
- Varicose veins, hernia.
Supermobility syndrome is usually diagnosed if you have:
- two main criteria,
- one main criterion and two secondary criteria,
- four minor criteria,
- two minor criteria and a close relative, such as a parent diagnosed with hypermobility syndrome.
Your doctor may also use blood tests and X-rays to rule out other diseases that may cause pain, such as rheumatoid arthritis.
Carter test
Content
- 1. History
- 2 Terminology
- 3 Pathogenesis
- 4 Classification
- 5 Clinical manifestations 5.1 Neurological impairment syndrome
- 5.2 Asthenic syndrome
- 5.3 Valve syndrome
- 5.4 Thoradiaphragmatic syndrome
- 5.5 Vascular syndrome
- 5.6 Thoradiaphragmatic heart
- 5.7 Arrhythmic syndrome
- 5.8 Sudden death syndrome
- 5.9 Bronchopulmonary syndrome
- 5.10 Visceral syndrome
- 5.11 Syndrome of pathology of the organ of vision
- 5.12 Hemorrhagic hematomesenchymal dysplasias
- 5.13 Foot pathology syndrome
- 5.14 Joint hypermobility syndrome
- 5.15 Vertebrogenic syndrome
- 5.16 Cosmetic syndrome
- 5.17 Mental disorders
Treatment
Treatment is not required if you have excessive joint flexibility that does not cause any symptoms.
However, you may need treatment if you have hypermobility syndrome, which causes symptoms such as pain. Doctors who treat hypermobility syndrome include general practitioners, family medicine doctors and internists, as well as rheumatologists and orthopedists.
Treatment is tailored to each person based on their specific presentation. Joint pain can be relieved with medications for pain or inflammation. A physical therapist with knowledge of hypermobility syndrome can be very helpful.
Physiotherapy can:
- reduce pain,
- improve muscle strength and performance,
- improve posture,
- improve your well-being,
- correct the movement of individual joints.
There are a number of physiotherapy techniques that are commonly used. For example, you may be given an exercise program that includes strength training, balance training, and specific stretching techniques.
How to treat vertebral hypermobility
Before treating vertebral hypermobility, it is necessary to identify the potential cause that provoked this disorder. If this is osteochondrosis, then before treating hypermobility of the cervical vertebrae, it is necessary to restore the performance of the muscles of the neck and collar area, improve the process of diffuse nutrition of the cartilage tissue of the intervertebral discs and eliminate all the negative consequences of the degenerative dystrophic disease.
The tactics for treating instability in the lumbosacral spine are constructed in a similar way. If the disease is associated with a violation of the integrity of the ligamentous and tendon apparatus, then it may be necessary to first undergo surgery to plasticize them.
In our manual therapy clinic, spinal hypermobility is treated using the following treatment methods:
- laser therapy – necessary in cases where there is tissue deformation and its integrity needs to be restored;
- electromyostimulation helps with insufficient development of the muscular framework of the back, neck and collar area;
- osteopathy and massage relieve excess tension in the muscles, enhance the process of microcirculation of blood and lymphatic fluid, increase the elasticity of soft tissues;
- therapeutic exercises and kinesiotherapy increase the tone of muscle tissue, improve the intensity of diffuse nutrition of cartilage and ligamentous tissue;
- physiotherapy accelerates metabolism at the cellular level, relieves swelling and inflammation.
The course of treatment is always developed individually, depending on the identified pathology, the patient’s health status, his age, weight, etc. Therefore, if you want to learn about the prospects for correcting spinal hypermobility in your individual case, then make an initial free appointment with a vertebrologist at our manual therapy clinic in Moscow. The form for making an appointment with a doctor is located further on the page.
Complications
Supermobility syndrome can be a problem for young people and adults. This is because of its possible complications.
Yes, hypermobility syndrome causes complications if the patient is not treated. Below is a list of complications and possible problems:
- chronic pain,
- chronic fatigue syndrome,
- fibromyalgia.
Due to the high mobility of the tissue, the joints wear out much faster. This causes constant injuries and sprains.
Story
Scientific and practical interest in joint hypermobility arose at the end of the 19th century, when hereditary syndromes were described, in the clinical picture of which joint hypermobility was one of the leading symptoms. Doctors of various specialties regularly saw patients who had structural non-inflammatory damage (often congenital or manifested at a young age) of individual organs or systems.
A group of hereditary diseases of connective tissue and skeleton was first identified by the American geneticist Mc Kusick in 1955. By that time, it united only a few nosological forms: osteogenesis imperfecta, Marfan syndrome, Ehlers-Danlos syndrome, elastic pseudoxanthoma and gargoilism.
Today, thanks to the achievements of genetics, over 200 diseases of the connective tissue and skeleton of a hereditary nature have been described and classified. [7]
Hypermobile metacarpophalangeal joint of the first finger
Hypermobile elbow joints
Consequences
A large proportion of hypermobility patients who follow joint protection recommendations do not suffer bone or joint damage as they age. However, some people with joint hypermobility may develop osteoarthritis, due to damage from recurrent dislocations or cumulative joint stress from long-term overactivity.
It is believed that men are less susceptible to hypermobility syndrome than women. Pathology has still been studied very little. Currently, various medical studies are being conducted in this direction. Let's hope that in the near future medicine will step forward, and this will enable people with excessively mobile joints to lead a normal life and play sports without fear for their health.
Clinical manifestations[ | ]
DST is a disease with very different clinical manifestations, from very mild in health to very serious and prognostically significant.
Valve syndrome[ | ]
Isolated and combined heart valve prolapse (most often mitral valve prolapse - 70%), myxomatous valve degeneration.
Thoraiphragmatic syndrome[ | ]
Asthenic shape of the chest, chest deformities (funnel-shaped, keeled), scoliosis.
Vascular syndrome[ | ]
Damage to elastic arteries: idiopathic expansion of the wall with the formation of a saccular aneurysm; damage to arteries of muscular and mixed types: bifurcation-hemodynamic aneurysms, dolichoectasia of elongated and local dilations of arteries, pathological tortuosity up to looping; damage to the veins (pathological tortuosity, varicose veins of the upper and lower extremities, hemorrhoidal and other veins); telangiectasia; endothelial dysfunction.
Thoraiaphragmatic heart[ | ]
Asthenic, constrictive, pseudostenotic, pseudodilation variants, thoraiaphragmatic cor pulmonale.
Arrhythmic syndrome[ | ]
Ventricular extrasystole of various gradations; multifocal, monomorphic, less often polymorphic, monofocal atrial extrasystole; paroxysmal tachyarrhythmias; pacemaker migration; atrioventricular and intraventricular blocks; anomalies in impulse conduction along additional pathways; ventricular preexcitation syndrome; long QT interval syndrome.
Bronchopulmonary syndrome[ | ]
Tracheobronchial dyskinesia, tracheobronchomalacia, tracheobronchomegaly, ventilation disorders (obstructive, restrictive, mixed disorders), spontaneous pneumothorax.
Visceral syndrome[ | ]
Nephroptosis and dystopia of the kidneys, ptosis of the gastrointestinal tract, pelvic organs, dyskinesia of the gastrointestinal tract, duodenogastric and gastroesophageal reflux, sphincter failure, esophageal diverticula, hiatal hernia; ptosis of the genital organs in women.
Syndrome of pathology of the organ of vision[ | ]
Myopia, astigmatism, hypermetropia, strabismus, nystagmus, retinal detachment, luxation and subluxation of the lens. Pathology of the cornea - keratoconus[7].
Hemorrhagic hematomesenchymal dysplasia[ | ]
Hemoglobinopathies, Randu-Osler-Weber syndrome, recurrent hemorrhagic (hereditary platelet dysfunction, von Willebrand syndrome, combined variants) and thrombotic (platelet hyperaggregation, primary antiphospholipid syndrome, hyperhomocysteinemia, factor Va resistance to activated protein C) syndromes.
Foot pathology syndrome[ | ]
Clubfoot, flatfoot (longitudinal, transverse), less commonly, hollow foot.
Joint hypermobility syndrome[ | ]
Joint instability, dislocations and subluxations of joints.
Vertebrogenic syndrome[ | ]
intervertebral hernia, spondylolisthesis, scoliosis, kyphosis, kyphoscoliosis.
Cosmetic syndrome[ | ]
Dysplastic-dependent dysmorphia of the maxillofacial region (bite anomalies, Gothic palate, pronounced facial asymmetries); O- and X-shaped deformities of the limbs; changes in the skin (thin translucent and easily vulnerable skin, increased skin extensibility, “tissue paper” suture).
Mental disorders[ | ]
Neurotic disorders, depression, hypochondria (including dysmorphophobia), anxiety-phobic disorders, anorexia nervosa.
Patients with DST form a group of increased psychological risk, characterized by a reduced subjective assessment of their own capabilities, level of claims, emotional stability and performance, increased levels of anxiety, vulnerability, depression, and conformism. The presence of dysplastic-dependent cosmetic changes in combination with asthenia forms the psychological characteristics of these patients: depressed mood, loss of a sense of pleasure and interest in activities, emotional lability, a pessimistic assessment of the future, often with ideas of self-flagellation and suicidal thoughts. A natural consequence of psychological distress is a limitation of social activity, a deterioration in the quality of life and a significant decrease in social adaptation, which is most relevant in adolescence and young adulthood.[8]
Mental disorders: also adaptation disorders, autism is possible.
Classification
Classification of DST is one of the most controversial scientific issues. The lack of a unified, generally accepted classification of DST reflects the disagreement of opinions of researchers on this issue as a whole. DST can be classified based on a genetic defect in the synthesis, maturation or breakdown of collagen. This is a promising classification approach that makes it possible to substantiate the genetically differentiated diagnosis of CTD, but to date this approach is limited to hereditary CTD syndromes.
Pathogenesis
DST is morphologically characterized by changes in collagen, elastic fibrils, glycoproteins, proteoglycans and fibroblasts, which are based on inherited mutations of genes encoding the synthesis and spatial organization of collagen, structural proteins and protein-carbohydrate complexes, as well as mutations in the genes of enzymes and cofactors for them. Some researchers, based on magnesium deficiency in various substrates (hair, red blood cells, oral fluid) detected in 46.6-72.0% of cases of DST, assume the pathogenetic significance of hypomagnesemia. [3]