Causes and mechanism of fracture
The main reasons why rib fractures occur include:
- Impact to the chest with a blunt object;
- Road traffic accidents;
- Falls from a height;
- Injuries during sports or physical activity;
- Squeezing;
- Rheumatoid arthritis;
- Primary tumors of bone marrow or bone tissue;
- Metastases of malignant neoplasms in bones;
- Genetic malformations of the skeleton;
- Osteoprosis.
Most often, injuries occur along the lateral surfaces of the chest in the area of greatest bend. The ribs from 4 to 7 are most susceptible to injury, since they are less elastic than those located below and are not protected in sufficient quantities by muscle tissue, like those located above.
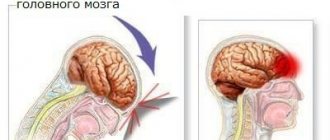
The fracture is often combined with damage to the parietal pleura and lung tissue, resulting in breathing problems, which poses a danger to humans.
I. Passport part. FULL NAME.:. Date of birth: August 23, 1929. Gender: male. Nationality Russian. Place of residence: city. Place of work: pensioner. Date and time of admission to the clinic: September 14, 2002, 12-00 hours. Referred to: city clinic No. 1, trauma center. Diagnosis: a) preliminary – fracture of the lower ribs on the left; b) clinical – fracture of the bodies of the VII-VIII ribs on the left. Concomitant diseases: type II diabetes mellitus, rhinophyma, chronic bronchitis.II. Patient complaints upon admission to the clinic. Pain in the left half of the chest, below, on the side and behind. The pain intensifies with deep breathing, coughing and when lying on the left side. Difficulty breathing due to pain. Difficulty in active movements due to increasing pain.
III. History of the disease. Mechanism and circumstances of injury. I was injured on the evening of September 13th. While rushing down the stairs in the dark, I slipped on the peel of a watermelon slice. Fell on his left side. I immediately felt pain in the places of impact, more intensely in the chest. However, at first he did not pay attention to the pain, assuming that it was associated with a bruise. During the evening, the pain in the chest on the left did not subside. He took analgesics on his own. Upon self-examination, I noticed a bruise at the site of the impact, which I attributed the pain to. Getting out of bed the next morning, I realized that the pain was not decreasing, it was associated with breathing, and the cough was very painful. Then I decided to go to clinic No. 1. After examination, the doctor was sent to the city hospital, traumatology department, where he was admitted, collecting his things and bedding.
IV. Anamnesis of life. He started walking and talking on time. I went to school at the age of 7. Education – 9 classes. Then he began serving in the army, as a driver in the border troops. Completed training at the sergeant's school. He served until 1953, then quit and began working as a driver. He retired due to old age in 1989. Didn't work in retirement. Has 3 children, all of them live in the Russian Federation. Widower. At school age he underwent appendectomy. Since 1986, he has been suffering from non-insulin-dependent diabetes mellitus and has been taking Maninil-5. He has been smoking since the age of 16 and drinking alcohol since the same age. Marks chronic bronchitis 21-22 years old. In 1934-35 (approximately) he suffered from malaria. He runs the household himself with the help of a neighbor who lives one floor down. Housework is considered feasible. Financial support – old age pension and assistance from children. Heredity is not burdened. Allergy history – population A.
V. General somatic status. The patient's condition is satisfactory. Consciousness is clear. The position is active, sparing the left side.
The skin is pink and flabby. Visible mucous membranes are of normal color. Rhinophyma is noted. The subcutaneous fat layer is somewhat overdeveloped. The food is satisfactory. Lymph nodes are not palpable, palpation is painless.
Respiratory system. Breathing through the nose, noisy, abdominal type. The chest is emphysematous, normosthenic. During the act of breathing, the left half of the chest is less mobile than the right. On palpation it is rigid, painful, especially on the left, vocal tremor is increased. During percussion, the sound over all the lungs is somewhat dull, but in the upper parts it is closer to the pulmonary one. Topographic percussion: right lung - lower edge anteriorly along the 7th intercostal space, lateral along the 7th rib, posteriorly along the 6th intercostal space; left lung - the lower edge in front along the VII rib, on the side along the VII rib, behind along the VI intercostal space. Standing height of the apexes: in front 3.5 cm above the clavicle, in the back along the spinous process of C6. The width of Krenig's fields is 4 cm. Mobility of the lower edges: right lung - 4 intercostal spaces, left lung - 3 intercostal spaces. On auscultation: breathing is harsh, in the upper parts of the lungs it is weakened. Diffuse abundant dry wheezing. BH 20 per minute.
Cardiovascular system: upon examination, the apex beat is invisible. The pulsation of the carotid arteries is barely noticeable. The neck veins pulsate slightly, barely noticeable at rest. Palpation: apex impulse in the 5th intercostal space 1 cm inward from the left midclavicular line (MCL). Percussion: OST - right border 1.7 cm outward from the right edge of the sternum, left - 1 cm inward from the left SCL, upper - on the third rib; borders of the AST - right - along the left edge of the sternum, left 1.5 cm medially from the left SCL, upper on the IV intercostal space. The diameter of the heart is 11.5 cm, the width of the vascular bundle is 5 cm. Auscultation: the tones are somewhat muffled, rhythmic. Heart rate 80 per minute. The pulse is symmetrical, regular, full, of normal tension. The walls of the arteries are thickened. A/D 130/80 mmHg. right, 140/90 mmHg. left.
Gastrointestinal tract: examination - the oral mucosa is pink, the tongue is covered with a white coating at the root and along the edges, the tonsils are not changed, there are 20 teeth, many are covered with metal crowns. There are no hernias or tumor-like formations noted in the abdominal area. A postoperative scar is found along the right inguinal fold. On palpation, the abdomen is soft, painless, the edge of the liver is smooth, even, painless. On percussion over the intestines there is tympanitis. Liver: upper border – VI rib along the parasternal line, VI rib along the right SCL, VII rib along the anterior axillary line; lower border - 6 cm below the xiphoid process along the midline, 0.5 cm below the lower edge of the costal arch along the left parasternal line, 2.5 cm below the lower edge of the costal arch along the right parasternal line, 0.5 cm below the edge costal arch along the right SCL, on the upper edge of the XI rib along the right anterior axillary line. The gallbladder is palpated at the intersection of the right rectus abdominis muscle with the costal arch and is painless. Auscultation: intestinal peristalsis is active, rhythmic, uniform.
Genitourinary system: examination - there are no tumor-like formations, the genital organs are developed according to the male type, secondary sexual characteristics correspond to age. Both testicles are palpable. The kidneys are not palpable. Pasternatsky's symptom is negative on both sides.
Endocrine system: the thyroid gland is homogeneous, not enlarged. There is no hyperpigmentation, ocular symptoms are negative. There is moderate obesity due to non-insulin-dependent diabetes mellitus.
Nervous system. Consciousness is clear, criticism of the state is preserved, oriented in time and space. Memory saved. Intelligence corresponds to age and education. The mood is even and cheerful. Behavior during questioning and examination is adequate. Falls asleep (according to the patient) quickly, 8-10 minutes after going to bed. Sleeps peacefully, without waking up. Dreams are ordinary and varied. Waking up in the morning is not difficult. There are no hallucinations, delusions, obsessive thoughts or actions. Speech is smooth and he pronounces words correctly. The vocabulary of the Russian language is sufficient. Understanding of the spoken speech is complete. There is no aphasia. There is no apraxia, agraphia, alexia, amusia, or acalculia. FMN: photoreaction is sluggish, convergence and accommodation are weakened. Hypermetropia and presbyopia are noted. There are no disturbances in the reflex, sensitive, or motor areas. Meningeal signs are negative.
VI. Status localis. Excursion of the chest on the left during breathing is limited. On the left, from the VI to IX ribs between the middle axillary and scapular lines, there is a large bruise and swelling. Palpation of the lower ribs is painful. When palpating the VII-VIII ribs, pain and bone crepitus are noted. You can feel the fracture line of the rib bodies.
VII. Preliminary clinical diagnosis . Fracture of the lower ribs on the left.
VIII. Paraclinical studies. 1. General blood test. 09.16.02 Hb 121 g/l; R 4.32 * 1012/l; CPU= 0.8; L 8.2 * 109/l; ESR 18 mm/h; leukocyte formula: young – 0; stab - 2; segmented – 67; eosinophils – 1; lymphocytes – 25; monocytes – 3.
2. Biochemical blood test. 09.16.02 Direct bilirubin – 0; indirect – 8.6; total protein – 67.7 g/l; blood sugar – 8.0 mmol/l.
3. General urine analysis. 09/16/02 Color – light yellow; transparency is not complete; relative density – 1018; protein – 0; L 2-4 in p/z; R 3-4 in p/z; squamous epithelium is single.
4. No worm eggs were found in the feces. Gregersen's reaction is negative.
5. ECG. Heart rate is 82 per minute, the rhythm is regular, sinus. The position of the electrical axes of the heart is horizontal. Signs of moderate right ventricular hypertrophy.
6. X-ray.09/14/02 Plain X-ray of the chest in the anterior projection: fracture of the bodies of the VII-VIII ribs on the left. Chronic bronchitis, vicarious emphysema of the upper lobes of the lungs. Hypertrophy of the right heart.
IX. Clinical diagnosis. Based on: complaints: pain in the left half of the chest, lower side and back, aggravated by deep breathing, coughing and when lying on the left side; difficulty breathing and active movements due to pain. medical history: I received the injury while going down the stairs in the dark, slipping on the peel of a watermelon slice and falling on my left side. I immediately felt pain in the places of impact, more intensely in the chest. During the evening, the pain in the chest on the left did not subside; it was associated with breathing; the cough was very painful. Then I decided to go to clinic No. 1. After examination by a doctor, he was sent to the city hospital, traumatology department; - clinical picture: rhinophyma is noted. Breathing is noisy, abdominal type. The chest is emphysematous, movement of the left half is limited. On palpation it is rigid, painful, especially on the left, vocal tremor is increased. During percussion, the sound over all the lungs is somewhat dull, but in the upper parts it is closer to the pulmonary one. On auscultation: breathing is harsh, in the upper parts of the lungs it is weakened. Diffuse abundant dry wheezing. BH 20 per minute. Cardiovascular system: tones are somewhat muffled. Heart rate 80 per minute; - status localis: the left half of the chest is less mobile than the right; on the left, from the VI to IX ribs between the middle axillary and scapular lines there is a large bruise and swelling. Palpation of the lower ribs is painful. When palpating the VII-VIII ribs, bone crepitus is noted; the fracture line of the rib bodies can be felt; paraclinical research methods: blood sugar – 8.0 mmol/l; Plain X-ray of the chest in the anterior projection: fracture of the bodies of the VII-VIII ribs on the left. Chronic bronchitis, vicarious emphysema of the upper lobes of the lungs. Hypertrophy of the right heart - a clinical diagnosis was made: closed fracture of the bodies of the VII-VIII ribs on the left. Concomitant diseases: type II diabetes mellitus, rhinophyma, chronic bronchitis.
X. Treatment. 1. Bed rest for 6 days; 2. blockade of the fracture site with novocaine 1% -10.0 once a day for 3 days; 3. ampicillin trihydrate 0.5 g 4 times a day for 5 days; 4. nicotinic acid 5% solution, 2.0 IM 1 time per day for 10 days; 5. vitamin B12 500γ, 1.0 IM 1 time per day for 10 days; 6. aloe extract liquid for injection, 1.0 IM 1 time per day for 10 days; 7. analgin 50% solution, 2.0 IM for severe pain; 8. Diphenhydramine 1% solution, 1.0 IM in one syringe with analgin for severe pain; 9. breathing exercises; 10. sollux on the left half of the chest.
Rationale for prescriptions: 1. bed rest to reduce the mobility of the patient’s axial skeleton and chest; 2. novocaine blockade of the fracture site relieves pain, reduces reflex tension of the intercostal muscles; 3. ampicillin trihydrate for the prevention of hematoma suppuration, in order to prevent congestive pneumonia; 4. nicotinic acid to dilate blood vessels and reduce post-traumatic swelling, improve nutrition of the ribs and damaged soft tissues; 5. vitamin B12 to improve metabolic processes; 6. liquid aloe extract for injection as an infiltrate-absorbing drug and biostimulant; 7. analgin solution to reduce pain, improve the patient’s condition, reduce anxiety; 8. diphenhydramine to reduce the patient’s anxiety due to pain, as a hypnotic; 9. breathing exercises to normalize lung function, prevent congestion in them associated with limited mobility of the chest; 10. Sollux to improve bone regenerative processes.
Recipes: 1. novocaine Rp.: Sol. Novocaini 1%-100.0 DtdN 3 S. for pain relief at sites of traumatic fractures (in the hands of a doctor!) # 2. nicotinic acid Rp.: Sol. Acidi nicotinici 5%-1.0 DtdN 20 in amp. S. 2 ml intramuscularly 1 time per day for 10 days. # 3. ampicillin trihydrate Rp.: Ampicillini trihyratis 0.25 DtdN 40 in tab. S. 2 tablets 4 times a day. #4. Vitamin B12 Rp.: Sol. cianocobalamini 500γ-1.0 DtdN 10 in amp. S. 1 ml intramuscularly 1 time per day for 10 days. #
5. aloe extract liquid for injection Rp.: Extr. Aloеs fluidum pro injectionibus – 1.0 DtdN 10 in amp. S. 1 ml intramuscularly 1 time per day for 10 days. # 6. analgin Rp.: Sol. Analgini 50% - 2.0 DtdN 10 in amp. S. 2 ml intramuscularly for severe pain. #7. Diphenhydramine Rp.: Sol. Dimedroli 1% - 1.0 DtdN 10 in amp. S. 1 ml intramuscularly with analgin in 1 syringe for severe pain. #
XI. Forecast and prevention. Prognosis: the patient’s age and concomitant diseases are complicating factors. However, the rib fracture was not accompanied by damage to the pleura or lung; treatment began 16 hours after the injury. Thus, the prognosis is favorable, restoration of working capacity will occur in 4-5 weeks. Prevention: preventing injuries, wearing appropriate glasses, moving more carefully.
XII. Diary. 09/24/02, 830 hours. A/D 130/80 mmHg, ps' 78. The patient's condition is satisfactory. Pain persists when coughing and palpating. Breathing is not difficult, there is no shortness of breath. The patient moves freely around the hospital.
09/26/02, 1800 hours. A/D 130/80 mmHg, ps' 76. The patient's condition is improving. Complaints of pain on palpation of the chest have practically disappeared. Pain persists when coughing and deep breathing. The patient spares himself. The food is ok. There are no minor complaints. At rest he does not feel pain, but cannot lie on his left side.
XIII. Epicrisis. The patient, born in 1929, was admitted to the clinic on September 14, 2002 and was under observation from September 24, 2002 to September 27, 2002. He was admitted with complaints of pain in the left half of the chest, below, on the side and behind, worsening with deep breathing, coughing and when lying on the left side. Difficulty breathing and active movements due to pain. From the medical history: he was injured on September 13, when he slipped while going down the stairs at home and fell. Took analgesics. The next day, he went to the emergency room of city clinic No. 1, from where he was sent to hospital treatment. From the life history: surgery for acute appendicitis, suffers from non-insulin-dependent diabetes mellitus, chronic bronchitis. Smokes, drinks alcohol. Objectively: signs of rhinophyma, chronic bronchitis, senile vicarious emphysema, moderate obesity due to diabetes mellitus. Status localis: left chest excursion during breathing is limited. On the left, from the VI to IX ribs between the middle axillary and scapular lines, there is a large bruise and swelling. Palpation of the lower ribs is painful. When palpating the VII-VIII ribs, pain and bone crepitus are noted. You can feel the fracture line of the rib bodies. A diagnosis was made: a closed fracture of the bodies of the VII-VIII ribs on the left. Concomitant diseases: type II diabetes mellitus, rhinophyma, chronic bronchitis. Treatment was prescribed and justified: 1. Bed rest for 6 days; 2. blockade of the fracture site with novocaine 1% -10.0 once a day for 3 days; 3. ampicillin trihydrate 0.5 g 4 times a day for 5 days; 4. nicotinic acid 5% solution, 2.0 IM 1 time per day for 10 days; 5. vitamin B12 500γ, 1.0 IM 1 time per day for 10 days; 6. aloe extract liquid for injection, 1.0 IM 1 time per day for 10 days; 7. analgin 50% solution, 2.0 IM for severe pain; 8. Diphenhydramine 1% solution, 1.0 IM in one syringe with analgin for severe pain; 9. breathing exercises; 10. sollux on the left half of the chest. By the end of the observation, the patient's condition improved: pain on palpation of the chest disappeared, the patient could move freely around the clinic, breathing became painless. It is recommended to complete the course of treatment and then try to prevent injuries.
Types of rib fractures
| According to the degree of rib damage | Crack | Minor rib injury |
| Complete fracture | The rib is damaged throughout its entire thickness | |
| Subperiosteal fracture | Bone damage occurs | |
| According to the degree of skin damage | Closed | There are no external signs of a fracture |
| Open | Skin is damaged | |
| By number of fractures | Unit | Damage to one rib |
| Multiple rib fractures | Several ribs are damaged, and the patient’s condition worsens, heart rate increases, breathing becomes shallow | |
| By location | Fenestrated rib fracture | The ribs are damaged on one side of the chest |
| Bilateral fracture | The ribs are damaged on both sides, and there is a possibility of respiratory problems | |
| Lateral and anterior fractures | The ribs are broken in the chest area or on the side. Severe injury accompanied by breathing problems | |
| Posterior fractures | Posterior rib fracture | |
| By presence of offset | With offset | The ribs become misaligned and can damage internal organs. |
| No offset | The ribs are in their normal position |
Anatomical features
The 12 pairs of ribs included in the structure of the chest serve as a shield for the respiratory organs and cardiovascular system. The curved plates are composed of osteochondral tissue. The posterior edges are connected to the spine, the anterior ones are connected to the sternum. The structure of the ribs is the same, the differences appear in the sizes and methods of connection.
The position of the ribs is maintained by adjacent muscles. 10 interlocking pairs form a ring for the internal organs. The lower 2 pairs are not connected to the sternum; they are called oscillating for their free retention on the muscles.
Among the upper and middle ribs there are:
- 1st to 7th true pairs connected to the sternum by cartilaginous tissue;
- 8th-10th false pairs connected by cartilaginous tissue to the upper arches.
The internal grooves of each costal arch contain neurovascular bundles. Damage violates their integrity, which causes sharp pain and disrupts the blood supply to organs.
The muscular system holds the rib frame. In the case of fractures, the displacement of fragments is rarely as significant as in other cases. But the risk of damage to other organs remains, especially with multiple injuries to the costal arches.
Symptoms of a rib fracture
The following signs may indicate a rib fracture:
- Pain in the area of the rib injury. Fragments of the ribs tear the intercostal muscles, irritate the nerve endings or the parietal pleura, which contains a large number of pain receptors. If the patient is at rest, the pain is dull and aching, but when coughing or inhaling it intensifies and becomes sharp. If the fracture is in the back of the ribs, the pain is less intense;
- Frequent shallow breathing. It is caused by severe pain in the affected area. If the patient tries to inhale forcefully, then at a certain moment the inhalation may be interrupted due to pain. If a large area of the chest or lung is damaged, respiratory failure may develop;
- A certain body position. To relieve pain, the patient leans towards the affected area or squeezes the chest with his hands, which makes it possible to reduce the amplitude of respiratory movements;
- Swelling and hematoma in the area of injury. An inflammatory reaction occurs, which causes swelling and blood accumulation;
- Deformation of the chest. The contours of the intercostal spaces are erased, and the chest in the affected area decreases in volume;
- Crepitus. A certain sound or tactile sensation that occurs when parts of a bone move relative to each other;
- Open wounds on the piles. In this case, bleeding may occur.
Rehabilitation
To speed up recovery, physiotherapy is performed. Folk remedies and home remedies are not the basis of treatment, but they help speed up rehabilitation. Shilajit has beneficial properties. It is used for rubbing. Traditional medicines include homemade ointments based on spruce resin. It stimulates repair and improves the condition of the musculoskeletal system.
As for useful physiotherapy procedures, the following are indicated for the formation of callus:
- UHF – relieves pain and swelling, accelerates the restoration of bone structures and cartilage tissue, improves nutrition of the affected area;
- UV irradiation – stimulates blood circulation, enhances repair and tissue metabolism, increases the absorption of vitamin D;
- amplipulse therapy – improves regeneration, stimulates bone tissue fusion, normalizes blood microcirculation;
- alternating currents – increase muscle tone, activate blood circulation. May be harmful in case of muscle hypertonicity.
At the same time, foods rich in calcium and dishes with gelatin are introduced into the diet. It is useful to eat pork ears and jellied meat, fermented milk products and fresh fruits. You can read more about nutrition for fractures here.
Therapeutic exercises are started only after the doctor’s approval. Loads are increased gradually. It is recommended to do exercises to activate general blood circulation, strengthen muscles and increase the flexibility of the spine. Due to the immobilization of the ribs, the spine suffers from a lack of mobility. Swimming is considered one of the safe and effective recovery methods.
Diagnostics
In order to diagnose an injury, the following methods are used:
- A clinical examination performed by a traumatologist or surgeon. He taps, examines and listens to the chest;
- X-ray of the chest cavity. It is quite informative and allows you to identify the number and location of fractures;
- Ultrasound examination of the chest. Allows you to identify blood accumulation in the pleural area;
- CT scan. Allows you not only to determine the presence of a fracture, but also to determine damage to internal organs.
How to determine a rib fracture
Diagnosis of a rib fracture involves radiography. A crack or break may be hidden behind an apparent bruise. It will not be difficult to see a rib fracture of any location on an x-ray. Examination of the bones provides comprehensive information, but does not say anything about the condition of the soft tissues.
If the X-ray information is not enough and a more detailed diagnosis is required, a CT scan is prescribed. This method allows not only to recognize bone destruction, but also associated damage.
How to find out which organs are affected by bone fragments? In this case, MRI is indispensable. To determine the condition of the heart, electrocardiography is prescribed.
First aid for broken ribs
What to do if a rib is broken: if you suspect a fracture, you should seek the help of a doctor. You should immediately call an ambulance if the patient has trouble breathing, bloody foam on the lips, feels dizzy, and loses consciousness.
- Before the ambulance arrives, the patient must be seated, reclining, with emphasis on the healthy part of the back . It is necessary to ensure that the patient does not lie down, since the sharp parts of the ribs can damage internal organs;
- The patient must be provided with fresh air;
- In order to relieve pain on the fracture area, you can apply ice and give the patient an anesthetic medication: Ibuprofen, Nimesulide, Ketanov, Analgin.
Rib fracture - symptoms, signs and treatment
A rib fracture is a less common traumatic injury than limb fractures. At the same time, this injury is often much more complex and dangerous than others due to its proximity to the ribs of the internal organs. In addition, it is not always possible to detect the problem immediately, which can also cause complications that are dangerous to the patient’s health in the future.
The treatment process takes a little time, but compliance with a special regime is mandatory.
Anatomy and structural features of the ribs
The bony frame that protects the internal organs in the upper torso (particularly the heart and lungs) from damage is called the rib cage. The chest, in turn, consists of twelve pairs of ribs, between which muscle tissue, nerves and vascular networks are laid.
In the back, the ribs are connected by the spine, in the front - by cartilage tissue. The cartilages, in turn, connect to the sternum and provide elasticity and some mobility to the costal plates.
If the chest is damaged, the integrity of one or more ribs, as well as soft tissues, skin and internal organs may be damaged.
Causes of fractures
The causes of rib fractures can be classified as mechanical and pathological. The first category includes the following factors:
- Road accident. Road accidents are the most common causes of rib fractures. As a rule, they occur when the chest hits the steering wheel, the asphalt, or when the body collides with the car body.
- Swipe. The bones of the chest are strong enough that significant force must be applied to cause a fracture upon impact.
- Industrial injuries. As a rule, fractures in this case occur due to strong compression. In severe cases, other parts of the body, including the skull, are damaged.
The second group includes predisposing factors that increase the fragility of cartilage and bone tissue. Among them:
- Rheumatoid arthritis;
- Malignant neoplasms that destroy bone tissue;
- Osteoporosis (in this case, a fracture is possible even with a weak mechanical impact);
- Rickets;
- Osteomyelitis;
- Genetic diseases and skeletal abnormalities.
Also, the cause of fragility of the chest can be congenital or acquired absence of the sternum. If there is a predisposition, patients should be constantly monitored by a doctor.
The answer to the question of how long it takes for a broken rib to heal directly depends on the patient’s compliance with the regimen and the doctor’s instructions. In most complicated cases, these periods are significantly longer than in normal situations.
Classification of rib fractures
Rib fractures are classified according to the following principles:
- Location. Injuries can occur on the right or left. Based on location, axillary, peri-scapular and peri-sternal fractures are distinguished.
- Degree of difficulty. Classify: fenestrated, single, double and multiple rib fractures.
- Presence of soft tissue damage. There are closed rib fractures (without breaking the integrity of soft tissues by fragmentation elements) and open (suggesting a violation of integrity).
- Location of fragmentation elements. A rib fracture can be classified as either displaced or non-displaced.
Traumatic injuries can be unilateral or bilateral. In addition, fractures can be complete, in the form of a crack, or subperiosteal (in this case, damage occurs only to bone tissue).
Mechanism of injury
Most often, rib fractures occur due to a strong blow or compression. In this case, the fracture is localized in the area of the greatest bend - along the lateral surfaces of the chest. Displacement during injury is rare, but multiple displaced fractures threaten significant damage to soft tissues and internal organs.
If a rupture of the lung or pleura occurs, complications arise in the form of pneumothorax (when air accumulates in the chest) and hemothorax (when blood accumulates between the outer and inner layers of the pleura).
There are other complications when the lung is damaged. Thus, air can penetrate the patient’s subcutaneous tissue and cause emphysema. Significant damage to the vascular network is usually accompanied by heavy bleeding into the soft tissue and pleural cavity.
Source: https://Sustavi.guru/perelom-rebra.html
Treatment of a rib fracture at home
The extent of medical care depends on the severity of the injury. First of all, the doctor assesses the patient’s condition and performs manipulations to maintain his vital functions.
At the initial stage, pain relief is performed by intramuscular administration of non-steroidal anti-inflammatory drugs.
Subsequently, the chest is immobilized. For this, the patient is seated and a pressure bandage is applied from a bandage, cut into strips of a sheet or towel.
For rib fractures, the bandage must be overlapped, as you exhale, and secured at the end . In this case, the muscles between the ribs do not participate in the act of breathing and the bone fragments do not move. The patient breathes through the diaphragm. The patient is transported to the destination while sitting.
After arriving at the hospital, assistance consists of several stages:
- Novocaine blockade. Allows you to temporarily reduce the sensitivity of nerve fibers in the fracture area. If it is not possible to make a blockade, the patient is administered narcotic analgesics: Tramadol, Nalbuphine;
- If the patient does not have concomitant pathologies, it is possible to apply a plaster cast to fix the chest. In other cases, elastic bandages are used;
- If several ribs are injured or there is a bilateral injury, the doctor may decide to install special plates that form the chest frame.
If the patient has an uncomplicated fracture of one or two ribs, then he can go home. At the same time, he must observe bed rest and sleep half-sitting until the condition improves. During this period, he needs to avoid physical activity and take non-steroidal anti-inflammatory drugs for pain relief: Diclofenac, Ibuprofen, Nimesulide.
In case of complicated fractures, the patient should be under the supervision of medical personnel , and bed rest should be extended to a month.
If complications develop, surgical intervention is performed.
First aid
Providing first aid for broken ribs by an amateur is unacceptable. The likelihood of complications, even death, is too high. First medical aid consists of immobilizing the victim and transporting him to the emergency room. In case of a closed injury, a non-narcotic pain reliever can be given.
The presence of pathological mobility of individual segments requires stabilization of the overall chest frame. This is achieved by applying a tight bandage, but assistance in case of rib fractures should only be provided by a doctor. Even incorrect application of the bandage can cause serious complications of the injury.
What to do if you have a broken rib
If one or two bones are injured, the victim can be taken to the hospital independently. Transportation for rib fractures is carried out in a sitting position. It is necessary to tighten the chest, but the breathing remains deep enough. Other transport immobilization is necessary for rib fractures with complications. The victim is transported in a reclining or lying position. For superficial wounds, an aseptic bandage must be applied.
Novocaine blockade can relieve pain. Anesthetize with a 1% solution of novocaine, which is injected into the intercostal nerves. In the case of a penetrating injury due to a rib fracture, first aid involves applying an occlusive dressing. The victim should lie correctly - on the healthy side or remain in a sitting position, if possible.
A traumatologist will explain what needs to be done in case of a rib fracture. He will also select the optimal position in which to transport a victim with rib fractures and carry out the following medical manipulations: puncture in case of high pressure in the pleural cavity, oxygen therapy in case of obstruction of the airway.
Only an experienced doctor will be able to take adequate measures and drain the victim if he has broken the sternum and damaged the pleura. When fluid accumulates between the pleural layers, the likelihood of respiratory failure increases, including complete respiratory arrest.
Complications
A rib fracture is dangerous precisely because of the complications it can cause:
- Pneumothorax. At the same time, air accumulates in the pleural cavity, which causes disruption of the lungs. It can be open when, as a result of the wound, the pleural cavity is connected to the external environment and the pressure in the lung drops. As a result, it completely disappears from the breathing process. With a closed pneumothorax, the lung tissue is damaged, and the air from it fills the pleural cavity and causes respiratory dysfunction. Any pneumothorax results in severe heart failure;
- Hemothorax. In this case, large blood vessels are damaged, and blood accumulates in the pleural cavity. On the affected side, breathing is impaired and the patient develops symptoms of internal bleeding;
- Acute heart failure. Occurs due to rupture of the heart wall or damage to large blood vessels. Blood accumulates in the pericardial cavity and the functioning of this organ malfunctions;
- Internal and external bleeding from arteries and vessels located in the chest cavity;
- Infectious complications. With an open fracture of the ribs, pathogenic microorganisms can enter the wound and cause an inflammatory process.
How does it manifest?
Symptoms of a rib fracture and the intensity of the clinical picture depend on the type of injury and the complication of impaired respiratory function. The main signs of a rib fracture:
- Painful sensations in the chest area;
- Increased pain when breathing;
- Swelling of tissues in the injured area;
- Hematoma;
- Subcutaneous hemorrhage;
- Crunch on contact;
- Coughing;
- The presence of blood clots in the sputum expelled when coughing;
- Subcutaneous emphysema.
Signs of a rib fracture are sometimes aggravated by injury to organs localized in the retroperitoneal space. In this case, a broken bone fragment puts pressure on the lung, and the fragment damages its integrity.
Pneumothorax
Complications of a rib fracture include:
- Pneumothorax is a condition in which the pleural membrane of the lung is injured with further penetration of air into it. Manifested by severe shortness of breath, acute pain, and heart rhythm disturbances. Without timely assistance, death inevitably occurs.
- Hemothorax is the penetration of blood into the pleura of the lung. Signs: shortness of breath, difficulty breathing, pain when inhaling.
- The development of heart failure - shallow breathing, the skin turns pale, the lips are bluish, the pulse quickens. During breathing, the chest sinks, one of its sides is located asymmetrically.
- Development of pleuropulmonary shock. The cause of the complication is extensive damage to the tissues of internal organs from fragments of broken bones with penetration of excess air into the pleura. The situation becomes more complicated when inhaling cold air. This complication is accompanied by symptoms of respiratory failure, a strong, suffocating cough, and the victim’s lower and upper extremities become cold.
Hemothorax
How to determine a rib fracture?
A doctor will be able to make a diagnosis after a medical examination, since, in most cases, if there is no displacement of fragments and damage to neighboring organs, clinical manifestations may be mild or blurred.
The greatest danger for patients is the floating type of rib fracture - separation of a bone segment from the chest area, damaging internal organs. Flotation in case of injury is characterized by severe pain, impaired respiratory function, and retraction of the sternum.
Stages of healing
Single uncomplicated fractures in children heal in 2–3 weeks. In older patients, this period extends to 3–5 weeks. Subsequently, the pain disappears and the person’s ability to work is restored.
Healing of the ribs occurs in several stages:
- Initially, cells forming a callus from connective tissue migrate to the point of injury with the blood flow;
- Then, inorganic substances and mineral salts accumulate inside this callus, forming an osteoid callus;
- Hydroxyapatites are deposited in the osteoid callus, which increase its strength.
Symptoms and signs
A rib fracture, especially a closed one, is not always immediately recognizable. Often, after a fracture, a person may not seek help for a long time , explaining the pain as a bruise from the blow.
Shallow breathing
When trying to take a full breath, a person with a fracture will feel pain. Therefore, he will breathe frequently and shallowly in order to disturb the chest less with movements.
Breast deformity
Upon detailed examination, even an inexperienced eye will notice the asymmetry and change in shape of the fracture site . To verify the presence of this symptom, you should examine the victim’s chest in different projections.
Crepitus
Crepitation is the characteristic sound of a bone crunching when light pressure is applied to the fracture site or an attempt is made to make a movement. This symptom should be checked carefully so as not to displace the fragments.
Interrupted breath
If you ask a person with a broken rib to take a deep breath, then in the middle of the breath he will abruptly stop and begin to breathe quickly and intermittently. This is called interrupted inspiration syndrome and occurs due to the sharp pain that appears when the fragments move.
Forced pose
In order to reduce suffering from pain, the victim unconsciously takes a position in which the fragments will move minimally and will not touch blood vessels and nerves. A typical position for a rib fracture is half-sitting, bending towards the side of the injury .
Other symptoms and signs
bruising at the fracture site . Loss of blood, pain and emotional stress cause pallor, dry mouth, and in severe cases, loss of consciousness.
Note! Of particular danger are fractures of the ribs with damage to the pleura (the thin lining of the walls of the chest and lungs). When the pleura is damaged, air enters the pleural cavity and compresses the lung (pneumothorax). The patient experiences difficulty breathing, dizziness, and oxygen starvation.
Rehabilitation after injury
In order to speed up recovery and avoid complications after a rib fracture, you must follow these rules:
- 3 weeks after injury, physical activity and physical activity are completely excluded;
- In the future, motor activity is gradually increased based on the patient’s perception of pain;
- You can return to sports no earlier than a month after the injury, and if the pain is insignificant. Ideally, this period should be increased to 8 - 10 weeks;
- In order to increase the amount of oxygen that enters the body and strengthen the muscles in the first 2 weeks after injury, it is necessary to perform breathing exercises, on the recommendation of your doctor;
If you suspect a rib fracture, you should immediately consult a doctor, as this is a fairly serious and painful injury.
If you follow all the specialist’s recommendations, you can return to normal life after a bruise within a month.
Treatment and rehabilitation
Restoration of ribs after a fracture in complicated injuries should take place under medical supervision in a hospital setting. It usually includes medication, physical therapy and surgical methods (if necessary). At the request of the patient and the capabilities of the medical institution, the use of alternative therapy is possible.
The following groups of drugs are used for treatment:
- anti-inflammatory;
- painkillers;
- immunostimulating;
- absorbable;
- wound healing;
- expectorants.
Treatment of complex rib fractures will require surgery.
If complications occur, rehabilitation after a rib fracture takes much longer.
To improve tissue nutrition, accelerate their regeneration, as well as normal resorption of callus, physiotherapeutic procedures are prescribed:
- microcurrents;
- medicinal electrophoresis;
- magnetic therapy;
- laser therapy;
- UHF.
To eliminate stagnant processes, hirudotherapy is considered an effective method of treatment, and acupuncture is used to eliminate pain and stimulate the body's defenses.
What treatment methods are there?
Treatment methods depend on the severity of the injury.
The severity of the fracture will determine the further treatment of the victim. An uncomplicated closed-type injury without concomitant damage to internal organs is treated with local anesthesia (novocaine or alcohol procaine blockade). The injection is given at the site of the fracture; if necessary, the injection can be repeated several times.
Next, the chest is fixed with a non-compressive bandage made of elastic bandages. Such fractures do not require hospitalization: to prevent congestion in the lungs, expectorants, breathing exercises, and physical therapy are prescribed for normal ventilation of the lungs.
Surgical intervention is required:
- for open wounds
- for pneumothorax (excess air is pumped out with a vacuum pump)
- with hemothorax (accumulated blood is removed from the pleura through a special tube)
- with multiple fractures and crushed ribs
In severe cases of fracture, surgeons restore the integrity of the chest and fix it using rigid fixation with plastic splints.
Wearing an orthopedic bandage also promotes rapid healing. It is produced separately for men and women, taking into account the peculiarities of the anatomical structure of the body.
Nimesil and Diclofenac are used as pain relievers; if there is a risk of infection or pneumonia, Amoxiclav or Ceftriaxone is prescribed.
Mechanisms of injury
The most common fracture of the ribs is 5-8 positions. And the most vulnerable place is the lateral part of the sternum, where the bones have the maximum bend. A very small percentage of damage occurs on ribs 9-15, as they are mobile enough to withstand external pressure.
A closed fracture of the back of the ribs can go unnoticed by the victim for a long time. Due to the low level of dynamics of bone fragments (and, accordingly, a blurred clinical picture), a person does not attach serious importance to his condition.
And injuries in the anterior section are especially painful, since when breathing and moving the bones become dynamic, causing severe pain. The symptoms of a rib fracture are very pronounced.
Under different traumatic conditions, a certain type of fracture inherent in a given situation will be observed:
- Local or limited. Occurs when a rib is impacted by a heavy and hard object with a limited area. Bone fragments are displaced inward.
- Full. The cause of such a fracture is a fall and landing on the sternum. In this case, the signs of a rib fracture are obvious, since a free bone fragment is formed, located near the pleura, pulmonary system, vascular network and nerves.
- Depressed. The broken fragment is pressed into the chest, damaging nearby organs and systems. This can happen with external pressure on the body, if the object exerting the impact has a large weight and area.
Classification
Regarding etiology, rib fractures are:
- Traumatic. When a short but powerful external effect is applied to a healthy bone.
- Pathological. When the bone structure is disrupted due to the course of the underlying disease. In this case, the fracture may be accidental.
Gradation of fractures relative to the mechanism of injury:
- Direct. The fracture site is localized at the point of direct exposure to the traumatic factor.
- Indirect. With angular displacement of the fragments. When a rib is struck closer to the spinal column, a violation of its integrity occurs in the form of a shear with the displacement of the peripheral fragment inward, while the main - central - fragment remains in place.
- Tear-off. With a significant displacement of the fragment relative to the rib. Similar injuries are typical for the IX and lower ribs.
Regarding skin damage:
- Closed: incomplete; full.
- Open: primary open; secondary open.
The difference between fractures regarding the nature of the damage:
- Isolated.
- Combined.
- Not heavy.
- Heavy.
- Polyfocal.
Depending on the nature of the fracture:
- Hammered.
- Longitudinal.
- Transverse.
- Compression.
- Oblique.
- Dentoform and others.
Regarding the existing fragments, their numbers and sizes:
- single-splintered;
- comminuted;
- finely fragmented;
- medium-fragmented;
- coarsely fragmented.
Types of fragment displacements:
- Primary.
- Secondary.
Regarding the spatial orientation of the debris:
- Widthwise, or sideways (lateral).
- By lenght.
- Along the axis (angular).
- On the periphery.
Gradation of rib fractures relative to the clinical condition:
- Stable.
- Unstable.
Diagnostic features
The clinical picture is not always obvious due to a number of signs. Then the fracture is determined using the symptom of axial load, that is, by squeezing the chest to increase the load on different parts. Pain occurs at the fracture site, not in the compression zone.
Correct palpation helps identify local pain. Comprehensive information including blood tests, urine tests, and X-ray results forms a holistic picture for an accurate diagnosis.
In general, the symptoms reliably reflect the nature of the damage and signal urgent measures to alleviate the condition or save the life of the victim.
Symptoms
Symptoms of a rib fracture may vary between single and multiple injuries. In this case, general signs are observed in each case:
- severe pain, the intensity of which increases when moving the body, deep breathing and coughing;
- difficulty breathing and local respiratory distress in the damaged area;
- edema;
- internal hemorrhage, expressed in the development of a hematoma;
- the characteristic sound of breaking bones, immediately following injury (may accompany the victim when trying to make active movements).
Signs of a rib fracture in several places at once or multiple fractures:
- subcutaneous emphysema (accumulation of air released as a result of lung damage);
- coughing with blood or bloody mass (a clear sign of a violation of the integrity of the tissues of the pulmonary apparatus).
- When palpated, the victim becomes especially painful, and the bones begin to move and make a faint crunching or “rubbing” sound.
Possible reasons
Elderly people are especially susceptible to rib fractures, since with age the elasticity of the chest deteriorates significantly and the bones become more fragile. However, such damage does not always depend on gender or age. The main reasons may be different:
- A blow directly to the chest when colliding with a hard surface. This can happen due to a collision or fall.
- Heavy objects falling on the chest. This happens when poorly fixed shelves, lighting elements or sports equipment fall.
- Strong compression of the chest from several sides at once also leads to disruption of the integrity of the ribs.
Most often, injuries occur as a result of car accidents, as well as in the process of domestic and industrial activities. The strength of the impact is indicated by the number of broken plates. Fractures of two ribs are not severe, since in most cases they do not lead to damage to internal organs.