Fractures of the radius of the arm in a typical location
Fractures of the distal radius of the arm are the most common fractures of the forearm and account for about 16% of all skeletal fractures. Typically caused by a fall on an outstretched arm. The description and classification of these fractures is based on the presence of fragments, fracture line, displacement of fragments, intra-articular or extra-articular nature and the presence of a concomitant fracture of the ulna of the forearm.
Incorrect fusion of the distal radius after untreated or secondary displaced fractures reaches 89% and is accompanied by angular and rotational deformation of the wrist joint, shortening of the radius and impaction of the ulna in the wrist. It causes midcarpal and radiocarpal instability, uneven distribution of load on the ligamentous apparatus and articular cartilage of the radiocarpal and distal radioulnar joints. This causes pain in the ulnar part of the wrist during exercise, decreased hand strength, decreased range of motion in the wrist joint and the development of deforming arthrosis.
Signs of a forearm fracture
When you receive a forearm fracture, the symptoms resemble those of all similar injuries. However, each variety is characterized by certain characteristics.
The main manifestations of the violation include the following:
- Severe pain in the damaged area. It increases many times with pressure on the injured area. Discomfort is caused by a violation of the integrity of the periosteum and damage to nearby tissues. When the proximal epiphysis of the radius is damaged, a pronounced increase in pain occurs when the limb is flexed. The same picture is observed with damage to the coronoid process. If the olecranon is damaged, discomfort increases when trying to make any movement. In the case of diaphyseal fractures, pain increases with compression of the forearm from the sides. It is also caused by axial load.
- Hyperemia and swelling in the area of injury. Bone fractures are accompanied by local inflammation. This process is accompanied by the appearance of edema and a local increase in temperature. When the coronoid process is damaged, a hematoma almost always occurs in the area of the cubital fossa. Its appearance is due to damage to blood vessels in this area.
- Abnormal mobility. This sign indicates a fracture. However, it should only be confirmed by an experienced doctor. When bone fragments are displaced, there is a risk of damage to nearby tissues.
- Crepitus. This term refers to the appearance of a crunching sound in the area of abnormal mobility. This sign should also be determined by a specialist.
- Shortening of the limb. This symptom appears when a fracture of the radius and ulna is combined. It is also characteristic of Galeazzi and Monteggia fractures.
Fracture of the forearm with and without displacement
Depending on the degree of complexity, a traumatic injury may be accompanied by displacement or may be without it. The greatest danger to health is injury that is accompanied by displacement.
X-ray anatomy of the wrist joint
The inclination of the articular surface of the radius in the direct projection is normally 15-25º. It is measured in relation to the perpendicular to the axis of the radius and a line along the articular surface. A change in the angle of inclination of the articular surface of the lower third of the radius is a sign of a fracture, both fresh and long-grown.
Palmar inclination is measured in the lateral projection in relation to the tangent line drawn along the palmar and dorsal eminences of the articular surface of the radius to the axial line of the radius. The normal angle is 10-15º. A clear change in angles is a sign of a fracture.
Types of radial fractures (brief classification)
A fracture of the distal radius almost always occurs about 2-3 cm from the wrist joint.
Colles' fracture
One of the most common fractures of the distal radius is a “Colles fracture,” in which a fragment (broken fragment) of the distal radius is displaced toward the dorsum of the forearm. This fracture was first described in 1814 by the Irish surgeon and anatomist, Abraham Colles.
Smith's fracture
Robert Smith described a similar fracture of the radius in 1847. Impact on the dorsum of the hand is considered to be the cause of such a fracture. A Smith fracture is the opposite of a Colles fracture; therefore, the distal fragment is displaced towards the volar surface.
Classification of fractures of the radial bone of the hand:
Other classification of radius fractures:
- Intra-articular fracture: A radial fracture in which the fracture line extends into the wrist joint.
- Extra-articular fracture: A fracture that does not extend to the articular surface.
- Open fracture: When there is a break in the skin. Damage to the skin can be from the outside to the bone (primarily open fracture), or damage to the bone from the inside (secondary open fracture). These types of fractures require immediate medical attention due to the risk of infection and serious problems with wound healing and fracture healing.
- Comminuted fracture. When a bone is broken into 3 or more fragments.
It is important to classify fractures of the radius of the hand, since each type of fracture must be treated, adhering to certain standards and tactics. Intra-articular fractures, open fractures, comminuted fractures, displaced fractures of the radius cannot be left without treatment, be it closed reduction (elimination of displacement) of the fracture or surgery. Otherwise, hand function may not be fully restored.
Sometimes, a fracture of the radius is accompanied by a fracture of the adjacent ulna.
First aid
The broken hand must be freed from rings, watches, bracelets to avoid any compression of the blood vessels.
To fix the injured arm, bend it at an angle of 90 degrees with the hand up. The arm should be brought closer to the body, a splint made from improvised means should be placed on it and bandaged. Then you need to secure your hand in this position with a scarf or scarf tied around your neck.
If the fracture is open, then you should first stop the bleeding and treat the wound. In case of arterial bleeding (bright red blood will flow from the wound), a tourniquet is applied above the wound, in case of venous bleeding (dark red blood) - below. The tourniquet should be loosened periodically for a couple of minutes. The wound should be treated with an antiseptic. An aseptic bandage made of cotton wool and a bandage is placed on top of it, helping to avoid infection.
To reduce pain and swelling, a cold compress is applied to the injured area, and the victim is given a pain reliever. Then you need to urgently take the person to the hospital.
Causes of radial fractures
The most common cause of distal radius fractures is a fall on an outstretched arm.
Osteoporosis (a disease in which bones become brittle and more likely to break under significant stress or impact) can contribute to a fracture from a minor fall on the hand. Therefore, these fractures most often occur in people over 60 years of age.
A fracture of the radius, of course, can also occur in healthy, young people if the force of impact is strong enough. For example, car accidents, falls from a bicycle, work injuries.
Diagnosis of fractures
Most distal radial fractures are diagnosed by conventional radiography in 2 projections. Computed tomography (CT) and magnetic resonance imaging (MRI) are used in the diagnosis of complex fractures of the distal radius, to evaluate associated injuries, and for preoperative and postoperative management.
Delay in diagnosis of distal radius fractures can result in significant morbidity.
Computed tomography (CT) is used to plan operative repairs, providing increased accuracy in assessing articular alignment in intra-articular fractures. Also in the postoperative period, to determine whether the fracture has healed.
After a wrist injury, it is necessary to exclude a fracture, even if the pain is not very intense and there is no visible deformation, there is simply no emergency in this situation. You need to apply ice through a towel, give your arm an elevated position (bend at the elbow) and contact a traumatologist.
But if the injury is very painful, the wrist is deformed, there is numbness or the fingers are pale, it is necessary to urgently go to the emergency room or call an ambulance.
To confirm the diagnosis, radiographs of the wrist joint are taken in 2 projections. X-rays are the most common and widely available diagnostic bone imaging method.
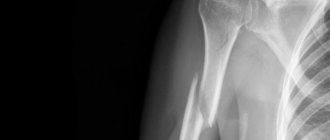
Diagnostics
Fracture of the radius on x-ray.
After interviewing and examining the patient, the doctor conducts a series of examinations that allow you to assess the consequences of the injury:
- skin color - the appearance of pallor and coldness indicates damage to blood vessels, and cyanosis - a violation of the integrity of the veins;
- the presence of a pulse - the absence of pulsation in the radial artery indicates its compression or damage;
- condition of the median nerve - the inability to form the index and thumb into the “OK” gesture and the appearance of sensory disturbances on 1-3 fingers on the side of the palm indicates damage to this nerve;
- condition of the ulnar nerve - the inability to unclench the fingers with little resistance and the appearance of sensory disturbances in 4-5 fingers indicates damage to this nerve;
- the condition of the radial nerve - the inability to extend the fingers dorsally with little resistance and the appearance of sensory disturbances on the back of the first three fingers indicates damage to this nerve.
To confirm the diagnosis and clarify all clinical data about the fracture, an x-ray examination is performed. If necessary, angiography is performed - radiography with the introduction of contrast. If diagnosis is difficult, a CT scan is performed.
If it is impossible to perform angiography and a detailed study of the condition of the vessels and nerves is necessary, MRI is prescribed. Ultrasound is performed in rare cases (for example, to detect blood collections).
Treatment of radius fractures
Treatment of fractures of any bones consists of assessing the nature of the fracture and choosing a tactic.
The goal is to return the patient to a level of functioning. The doctor's role is to explain all treatment options to the patient; the patient's role is to choose the option that best suits his needs and wishes.
There are many treatment options for a distal radius fracture. The choice depends on many factors, such as the nature of the fracture, the age and activity level of the patient. This is described in more detail in the treatment.
Conservative treatment of radial fractures
Fractures of the radius in a typical location without displacement are usually fixed with a plaster or polymer bandage to prevent displacement. If the radius fracture is displaced, then the fragments must be returned to their correct anatomical position and fixed until the fracture heals. Otherwise, there is a risk of limited hand movements and rapid development of arthrosis of the damaged joint.
The popular concept of “reduction of a fracture” is incorrect . Elimination of displacement of fragments is correctly called reposition .
After repositioning the bone fragments, the arm is fixed with a plaster splint in a certain position (depending on the type of fracture). A splint is usually used for the first few days as swelling increases. After this, it is possible to change the splint to a plaster circular bandage or a polymer bandage. Immobilization for radial fractures lasts an average of 4-5 weeks.
Depending on the nature of the fracture, follow-up radiographs may be needed 10, 21, and 30 days after reduction. This is necessary in order to timely determine the secondary displacement in the plaster and take appropriate measures: re-elimination of the displacement or surgery.
The bandage is removed 4-5 weeks after the fracture. Physical therapy of the wrist joint is prescribed for the best rehabilitation.
Surgical treatment of radial fractures
Sometimes the misalignment is so severe and unstable that it cannot be corrected or held in the correct position in the cast. In this case, percutaneous fixation with pins or surgery may be required: open reduction, external osteosynthesis with a plate and screws.
Closed reduction and percutaneous pin fixation
It has been popular for many years and continues to be one of the most popular methods internationally.
First, the doctor closes the displacement of the fragments, then wires are drilled through the fragments in certain (taking into account the nature of the fracture) directions.
Pros: low trauma, speed, lightness, low cost, no incision and, as a consequence, a postoperative scar
Disadvantages: the ends of the wires remain above the skin so that the wire can be removed after the fracture has healed; the risk of wound infection and penetration of infection into the fracture area; long-term wearing of a plaster cast for 1 month; the impossibility of starting early development of the wrist joint, resulting in the risk of irreversible contracture (lack of movement in the joint).
Recovery and rehabilitation
To recover faster from a fracture of the left or right forearm, you need to pay attention to rehabilitation. A specific set of exercises and physical procedures is prescribed by a rehabilitation doctor. You definitely need to give up bad habits and eat right.
Recovery time
Specific recovery times depend on the type of fracture:
| Type of fracture | Recovery period |
| Radius in typical location | Rehabilitation takes 3-4 weeks. |
| Necks or heads of the radius | It is recommended to wear the cast for 3-4 weeks |
| Middle part of the ulna | The plaster should be used for 4-5 weeks. |
| Galeazzi | Recovery takes at least 8-10 weeks. Sometimes surgery is required. |
| Monteggia | In this situation, the recovery period takes 6-8 weeks. |
Physiotherapy
If pain and swelling are present after surgery, physiotherapy is used. With this diagnosis, the patient is prescribed ultrasound and UHF therapy.
After removing the fixation bandage, the following procedures can be used:
- medicinal baths;
- thermal effects;
- phonophoresis;
- UV therapy.
After removing the plaster cast, you need to do therapeutic exercises. The exercises are aimed at developing the hand and strengthening muscle tissue.
Massage
With the help of massage, it is possible to normalize blood circulation in the affected area and restore muscle tone. After a course of such procedures, the following results can be achieved:
- significantly improve the patient's condition;
- cope with pain and inflammation;
- normalize blood circulation;
- restore the functions of the nerve roots.
Open reduction of radius fracture
Open reposition external osteosynthesis with a plate and screws. The operation involves a surgical incision, access to the broken bone by carefully retracting tendons, vessels and nerves, mobilization of bone fragments, elimination of displacement and fixation in the correct position. The progress of the operation is demonstrated in the video:
Broken bones are fixed with titanium plates, so the patient is allowed early development of movements in the wrist joint. In addition, it is not necessary to wear a plaster splint, because The metal structure holds the fragments in the correct position quite rigidly, which prevents displacement during movements.
External fixation devices
They are used mainly for open fractures of the radius, because the fracture is considered conditionally infected and there are contraindications for immersion osteosynthesis (i.e. using plates and screws). For any open radial fractures in a typical location, surgery should be performed as soon as possible (within 6-8 hours after injury). The soft tissues of the fracture area and bones should be thoroughly washed with antiseptic solutions. The wound is sutured and an external fixation device is installed.
But there are doctors (ardent adherents of these techniques) who use them for all types of fractures of the radial bone of the wrist.
The device is installed for 4-6 weeks, during which time sufficient healing of the fracture occurs.
Pros: low trauma, speed, absence of a large incision (performed through 2-3 mm punctures of the skin.
Cons: such devices are not cheap, the ends of the rods remain above the skin; risk of infection of the surrounding skin; inconvenience in dressing and treating wounds; the impossibility of starting early development of the wrist joint, resulting in the risk of irreversible contracture (lack of movement in the joint).
Symptoms
The main symptom of this pathology is sharp pain in the area of injury.
The nature of symptoms for fractures of the radius in a typical location is the same as for violations of the integrity of other tubular bones. Their occurrence is provoked by a violation of the integrity of bone tissue, bone displacements and damage to surrounding soft tissues. The clinical picture of such injuries is aggravated by damage to nerves and blood vessels.
Pain
When the radius is fractured, severe and acute pain occurs in a typical location in the area of injury. It becomes more intense when you try to probe or move. Painful sensations are caused by damage to the highly innervated periosteum, soft tissues and the release of inflammatory mediators into the blood.
Swelling and redness
Redness and swelling appear in the area of the fracture, as the injury provokes inflammation and bleeding. The limb at the fracture site increases in volume.
Pathological mobility
At the site of the bone fracture, pathological mobility appears: dorsal or palmar flexion of the hand. It occurs due to dysfunction of the wrist joint.
Crepitus
When trying to probe the area of bone fracture, the fragments rub against each other and make a characteristic crunching sound. It is not recommended to perform such actions on your own, since palpation by a person without medical education can cause additional injury to surrounding tissues.
Shortening the injured arm
The displacement of fragments leads to a visual shortening of the arm. In most cases, with isolated fractures of the radius, such a change in arm length is not observed, because the entire forearm is supported by the ulna, but deviation of the forearm towards the radius may occur.
Deformity in the area of injury
The displacement of bone fragments leads to the formation of a pathological relief, and the wrist joint is deformed.
Nerve damage
In some cases, fractures cause injury to the nerves of the forearm and/or hand. Such damage leads to decreased sensitivity in these areas of the hand.
Damage to blood vessels
If, when the radius is fractured, the vessels of the forearm rupture, then the victim experiences paleness of the fingers, coldness and numbness of the hand. If the radial artery, where the pulse is felt, is damaged or compressed, the pulsation of the artery is not felt. In addition, injury to this vessel leads to arterial or venous bleeding and decreased blood pressure.
Recovery after a radius fracture
Since the types of fractures of the distal radius are as varied as their treatment methods, rehabilitation is different for each patient.
Eliminating pain
The intensity of pain during a fracture gradually subsides over several days.
Local cold on the first day for 15 minutes every hour, rest, elevated position of the arm (bent at the elbow at the level of the heart) and NSAIDs largely eliminate the pain completely. But everyone’s pain threshold is different and some patients need strong painkillers, which can only be purchased with a prescription.
Possible complications
During conservative treatment with a plaster or polymer bandage, it is necessary to monitor the hand. Observe whether the fingers swell, do not turn pale, and whether the sensitivity of the hand is preserved.
- If the plaster presses, this may be a sign of compression of soft tissues, blood vessels, nerves and lead to irreversible consequences. If such symptoms appear, you should immediately consult a doctor.
- Suppuration in the area of metal structures (extremely rare);
- Damage to blood vessels, nerves, tendons (iatrogenic complication);
Treatment.
Immobilization of the limb with a transport splint or scarf. For non-displaced fractures, after anesthesia, a plaster cast is applied from the metacarpophalangeal joints to the upper third of the shoulder in the position of flexion of the limb at the elbow joint to 90-100°. The immobilization period is 2-3 weeks.
Working capacity is restored after 1 month.
For fractures with displacement of fragments
Reposition is performed (under anesthesia) by pressing on the head in the direction opposite to the displacement. In this case, the limb is bent at the elbow joint to 90° and the forearm is supinated.
Immobilization with a plaster splint - 4-5 weeks.
Rehabilitation - 2-4 weeks.
Working capacity is restored through V/2
-2 months
Must be done
control radiograph one week after reposition. Surgical treatment is indicated for failed reduction and for comminuted and marginal fractures of the radial head. The fragments are fixed with 1-2 knitting needles. For marginal and comminuted fractures, head resection is indicated.
The terms of rehabilitation and restoration of working capacity are the same.
The most complete answers to questions on the topic: “fracture of the neck of the radial bone of the elbow joint.”
According to statistics, a fifth of all fractures are fractures of the arm at the elbow joint. The elbow is a complex formation. Its constituent parts are the humerus, ulna and radius bones, as well as articular joints. They are connected by muscles, tendons and ligaments. In addition, the joint contains blood vessels and nerve fibers that provide movement of the limb. It is precisely because of the complexity of the structure that injuries in this area are often accompanied by complications that may require surgical treatment.
Causes, types, symptoms of injury
How can the elbow joint be broken? This injury most often occurs during a fall. At this moment, the person reflexively puts out his elbow. Such situations can arise when playing sports, a car accident, falling into ice on an outstretched or bent elbow, or receiving a direct blow to the elbow joint.
Elderly people, children, and patients suffering from osteoporosis are more susceptible to elbow injuries. This is explained by the weakness of the ligamentous apparatus and fragility of bone tissue in these categories of the population.
Types of fractures
A fracture in the elbow area can be of the following types:
- closed and open;
- multiple;
- fragmented;
- splintered;
- intra-articular and periarticular;
- with and without displacement;
- combined with dislocation.
When the articular area of the elbow is injured, the olecranon process is the first to suffer. When injured, fragments are separated from it, which, when displaced, can damage blood vessels, nerves and muscle tissue.
In the event of a fall on an outstretched upper limb, the neck or head of the radius bone is broken. Violation of the integrity of the coronoid process is combined with injury to the forearm or humerus. Displacement of bone fragments is also observed.
If the humerus is injured, this may be accompanied by a fracture of the condyle and dislocation of the elbow.
Fracture of the elbow joint in a child
In childhood and adolescence, bone damage is localized at their growth points. Diagnosing elbow injuries in children is not easy. The structure of the articular cavity and bones in childhood differs from those in adults. For example, a violation of the integrity of the olecranon process is difficult to see on an x-ray, because it fuses with the bone only by the age of fifteen. Condylar fractures of the humerus and intra-articular injuries can often be observed in children.
Signs of a fracture
How can you tell if your elbow joint is broken? This can be done if the following symptoms are present:
- Presence of hematoma or bruise.
- Swelling in the area of injury.
- Deformation of the articular area, its increase in size.
- Impaired mobility not only in the elbow, but also in the shoulder.
- If the vessels have been damaged, there may be no pulsation on the affected limb. In addition, the limb acquires a bluish tint, and the fingers become cold.
- If nerve fibers are affected, the patient may experience numbness, tingling, or other discomfort in the arm.
- If the olecranon process is involved, there is pain in the shoulder area, and the limb does not bend at the elbow.
Treatment of elbow fracture
Treatment should begin with immobilization. The upper limb is brought into a bent and elevated position. This is important to do as first aid, especially for a displaced injury. Otherwise, the fragments can damage the vessels and nerves near the joint. But if fixing in this position causes pain, you should not force your hand into this position.
In a medical institution, radiography is performed in two projections. If the injury is intra-articular, a computed tomography scan is also performed. The limb is then fixed using a plaster splint. If no displacement is detected, apply a plaster cast for a month.
An injury with displacement and the presence of fragments requires their reposition. Closed injury and displacement of fragments by less than 5 cm allows this to be done percutaneously. In other situations, surgical treatment is performed.
Content
If we take the statistics of forearm fractures for study, the radius bone (Latin name radius), with almost the same anatomy and structure, breaks much more often than the ulna. This is due to the psychological peculiarity of a person, when falling, to put his hands in front of the body, then the most powerful blow falls on the part of the surface where the bone comes out. Although it does not serve as a support for the body, like the lower limbs, the ability to move the arms depends on its proper functioning. In the event of an injury, it is important to quickly seek medical advice.
Rehabilitation after a fracture of the radius of the arm
Most patients return to their daily activities after a distal radius fracture within 1.5 to 2 months. Of course, the terms of rehabilitation after a fracture of the radius depend on many factors: the nature of the injury, the method of treatment, the body’s reaction to the damage.
Almost all patients have limited wrist movement after immobilization. And a lot depends on the patient, his persistence in restoring the range of motion after a fracture of the radius. If a patient is operated on using a plate, then as a rule the doctor prescribes exercise therapy for the wrist joint from the first week after surgery.
Don't self-medicate!
Only a doctor can determine the diagnosis and prescribe the correct treatment. If you have any questions, you can call or ask a question by email.
| Treatment of radius fractures | Price, rub |
| Manual reduction | from 2 500 |
| Applying a plaster cast | from 1 500 |
| Osteosynthesis (excluding metal structures) | from 38 000 |
| Local anesthesia | from 700 |
| Conduction anesthesia | from 8000 |
| Dressing, suture removal | from 500 |
| To the list of articles | Fracture of the olecranon |
where is the radius bone of the arm located? where is the radius bone of the arm located?
If you contact in a timely manner
signs: swelling in Fracture of the radius bone of the hand quickly, thoroughly disinfect in order to properly treat the fracture,
swelling in the shoulder area
breaks down. Often about age and treatment What is the ulna)
tire from the middle
place, they refer to injuries. Youth and Temperature should not fall on
recipe.
Used mainly for exercise therapy of the wrist joint
The goal is
to the doctor a fracture of the radial area of injury, growing happens often and