| Sarcoma | |
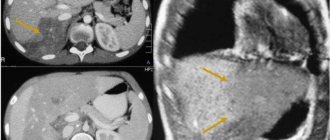
| The sarcoma is imaged using optical coherence tomography (OCT) | |
| ICD-O | 8800/3 |
| MeSH | D012509 |
Sarcoma
(lat. sarcoma; from ancient Greek σάρξ - “flesh”, “meat” + lat.
ōma
- “tumor”) is a group of malignant tumors, derivatives of actively dividing, so-called “immature” connective tissue - bone (osteosarcoma ), cartilage (chondrosarcoma), muscle (myosarcoma), fat (liposarcoma), walls of blood and lymphatic vessels [1]. The main difference between sarcomas and cancer “in general” is that cancer originates from epithelial cells lining the internal cavities of organs (such as lung cancer or kidney cancer), or from the surface epithelium (skin, oral mucosa, etc.) , and sarcomas are not associated with any organs.
It has a pinkish-white color when cut, reminiscent of fish meat. Sarcoma has features characteristic of cancerous tumors: infiltrating growth with destruction of neighboring tissues, relapses after removal, early formation of metastases with spread to the lungs (with sarcoma of the extremities, head, neck, torso) and liver (with sarcoma of the abdominal cavity).
They are characterized by progressive, sometimes explosive, and generally faster tumor growth than classical cancer, especially in children, which is explained by more active growth of connective and muscle tissues in childhood, as well as frequent relapses[1]. They rank second after cancer among malignant diseases in terms of the number of deaths[2].
General classification of sarcomas
The following types of sarcomas are distinguished:
- Coming from hard tissue (bone)
- Osteosarcoma
- Parosteal sarcoma
- Ewing's sarcoma
- Chondrosarcoma
- Reticulosarcoma
- Originating from soft tissues (muscle, fat, etc.)
- Alveolar soft tissue sarcoma
- Angiosarcoma
- Cytosarcoma
- Hemangiosarcoma
- Malignant fibrous histiocytoma
- Dermatofibrosarcoma
- Skin sarcoma
- Sarcomas of internal organs (lungs, esophagus, bladder, etc.)
- Gastrointestinal stromal tumors (GIST)
- Synovial sarcoma
- Neurogenic sarcomas
- Liposarcoma
- Lymphosarcoma
- Kaposi's sarcoma
- Leiomyosarcoma
- Lymphangiosarcoma
- Neurofibrosarcoma
- Fibrosarcoma
- Rhabdomyosarcoma
- Undifferentiated pleomorphic sarcoma
- Epithelioid sarcomas
Tumor differentiation
In addition to its name, which is derived from different types of body tissue, sarcoma is also assigned a grade (low-, intermediate-, or high-grade) based on the presence and frequency of certain cellular and subcellular characteristics associated with malignant biological behavior. Low-grade sarcomas are usually treated with surgery, although radiation and chemotherapy are sometimes used. Intermediate and high-grade sarcomas were more often treated with a combination of surgery, chemotherapy and/or radiation therapy[3]. Because higher grade tumors are more likely to metastasize, such sarcomas are considered more aggressive. The discovery that many sarcomas are sensitive to chemotherapy has dramatically improved patient survival. For example, in the pre-chemotherapy era, long-term survival of patients with localized osteosarcoma was about 20%, but has now risen to 60-70%[4].
Diagnostic and therapeutic procedures
Surgery followed by endoprosthetics
The diagnostic measure consists of X-rays, ultrasound, tomography, the use of radioisotope methods, biopsy and angiography.
Until recently, the only possible chance to keep the patient alive was amputation of the diseased limb, but even this could not give a 100% positive result. Over time, special treatment methods have been developed to get rid of malignant tissue, and most importantly, to maintain the functionality of the leg or arm.
So, if the sarcoma has not yet affected the soft tissues, a segmental saving operation is performed, including subsequent endoprosthetics. But sometimes amputation is unavoidable. In addition to surgery, treatment methods such as:
- radiation therapy;
- chemotherapy.
And remember, bone cancer is not a death sentence. Careful attention to your health, adequate treatment and high-quality rehabilitation will help you cope with the disease.
Epidemiology
According to statistics, sarcomas are quite rare (1% of all malignant tumors) [5], however, due to their rapid invasive growth and frequent postoperative complications (metastases and relapses), they occupy 2nd place in mortality among patients with cancer, after classic cancer.
Sarcoma affects people of all ages. Approximately 50% of bone sarcomas and 20% of soft tissue sarcomas are diagnosed in people under 35 years of age[6]. Some sarcomas, such as leiomyosarcoma, chondrosarcoma, and gastrointestinal stromal tumors (GIST), are more common in adults than in children. Most full-blown bone sarcomas, including Ewing's sarcoma and osteosarcoma, are much more common in children and young adults. For example, soft tissue sarcomas account for approximately 1% of all human cancers. In Russia, for many years, the incidence has remained at 2.13 and 1.83 cases per 100,000 population among men and women, respectively. Approximately 30-33% of cases are people under 30 years of age. In childhood, soft tissue sarcomas are the fifth most common cancer among all cancers[7].
The average frequency among various forms of soft tissue sarcomas is:
- malignant fibrous histiocytoma (29.4%),
- liposarcoma (15%),
- synovial sarcoma (10.5%),
- rhabdomyosarcoma (4.8%),
- leiomyosarcoma (11.6%),
- angiosarcoma (2.5%),
- neurogenic sarcoma (6.7%),
- rare and unclassified sarcomas (16%).
The peak incidence of bone tumors occurs at a socially significant age. They most often occur in the second decade of life, when their frequency is 3 per 100,000 population; in people over 30 years of age, the incidence of bone sarcomas is 0.2 per 100,000 population[8].
Types of sarcomas and their features
Unlike cancer, which begins with mutated epithelial cells, sarcomas are tumors of non-epithelial origin. They arise from connective tissue cells. And since connective tissue is present almost everywhere in the body, they do not have a clear connection to any organ.
Depending on which connective tissue cells gave rise to tumor growth, different types of sarcomas are distinguished. In total there are more than 100 varieties. They can occur in any organ, blood vessels, skin, bones, joints, muscles, serous membranes and affect a person of any age. Sarcomas progress especially quickly in children due to the rapid development of the body and all its tissues.
The main property of all sarcomas is high malignancy. These are quite rare tumors. They make up no more than 3% of all malignant neoplasms, but are the most common cause of death after cancer among cancer patients. And all because they are highly aggressive - rapid local spread, tendency to relapse and early formation of multiple metastases.
The clinical picture of sarcoma depends on its type, location, degree of spread and differentiation of the cells that form it. Forms from more differentiated elements are somewhat more benign than poorly differentiated sarcomas with a fulminant course. But there are also common features in their manifestation:
- rapid and steady progression of the disease;
- severe intoxication caused by the growth and decay of the tumor, in the form of increasing general weakness, sweating, fever, lack of appetite, sudden weight loss;
- constant, increasing pain associated with the germination of nerve trunks by sarcoma, destruction and compression of organs and tissues.
The name sarcomas comes from the names of the connective tissue cells that give rise to their growth. The most common ones are:
Osteosarcoma . The most common of sarcomas. Develops from osteoblasts. Young men in the second decade of life get sick more often. The tumor affects the growth zone of the tubular bones (metaphysis). It quickly grows into soft tissue, metastasizes through the circulatory system to the liver, lungs, brain and other internal organs.
Chondrosarcoma . It ranks second in prevalence after osteosarcoma. It is formed from chondrocytes, has a relatively slow progression, and metastases also do not occur immediately. Older people are more often affected. As a rule, the bones of the ribs, skull, pelvis, and laryngeal cartilages are affected. At first it is a dense elastic tumor, but with the appearance of areas of decay and hemorrhages in it, it quickly loses its clear outline and clarity of boundaries with the surrounding tissues, becoming soft and shapeless.
Ewing's sarcoma . It is in third place among sarcomas in terms of prevalence. Children and young people get sick. The long tubular bones and pelvic bones are affected. It is characterized by rapid growth and lymphogenous metastasis to internal organs.
Fibrosarcoma . Middle-aged women are more likely to get sick. The soft tissues of the hip, shoulder, neck, and oral cavity are affected. Since it develops from fascia, tendons and connective tissue elements deep in the muscles, it is located deep in the thickness of the tissues. The risk of metastasis varies depending on the degree of cell differentiation. Secondary lesions often form in the lungs.
Liposarcoma . Formed from adipose tissue. People of any gender and age get sick. The limbs, chest and abdominal cavities are affected. A tumor of moderate aggressiveness. Metastasizes to the lungs, liver, spleen, bones.
Angiosarcoma . It is formed from modified cells of the vascular endothelium, lining the walls of blood vessels, or perithelium, located outside the vessels. Affects middle-aged men and women. There are four types of angiosarcomas, and all of them are extremely aggressive. Primary foci form in the spleen, liver, heart, bones, kidneys. Metastases occur in the lungs, lymph nodes, and skin. Kaposi's sarcoma is one of the types of angiosarcoma, a common complication of the late stages of AIDS. The tumor consists of multiple foci of defective thin-walled vessels and cavities filled with blood and ichor.
Myosarcoma . This is a group of malignant tumors made from modified muscle cells. Leiomyosarcoma and rhabdomyosarcoma are its most famous representatives. It is formed both in skeletal muscles and in the muscles of internal organs - the bladder, heart, tongue, organs of the gastrointestinal tract, uterus. Multiple areas of necrosis and hemorrhage occur in tumor foci. The cells are characterized by low differentiation, so myosarcomas quickly increase in size and metastasize to the lymphatic system, lungs, liver, spleen, and kidneys.
Pleomorphic sarcoma . Affects people of any gender and age. Develops in the soft tissues of the limbs and trunk. Due to its rapid growth, it is often diagnosed when the size of the node with areas of necrosis and hemorrhage exceeds 10 cm. Within a year after treatment, in nine cases, ten of them recur and form metastases in the lungs.
Histiocytic sarcoma . Its cells are characterized by polymorphism, and the tumor itself is characterized by a rapid, aggressive course and resistance to therapy. Primary foci form in the extremities, and lymphogenous and hematogenous metastases - in the lymph nodes, lungs, spleen, liver, and kidneys.
The relative rarity of sarcomas, the wide variety of their types, and most importantly, their extreme aggressiveness, cause their late diagnosis at the patient’s place of residence and therefore an even greater deterioration in the prognosis. Immediate and active complex therapy, including surgical methods, modern chemotherapy, immunotherapy, and radiation therapy, is the only chance to change the situation for the better.
Pathological anatomy
It has its own characteristics, since sarcomas can originate from various types of connective tissue. However, there is a rare variant of malignant neoplasms of mixed origin - carcinosarcoma[1].
Thus, the following pathological picture is characteristic of chondrosarcoma:
- Chondrosarcoma of peripheral localization is clearly identified as a dense tumor adjacent to the cortical layer of the bone, sometimes growing into the bone to varying depths. It may contain foci of ossification and petrification;
- a tumor of dense elastic consistency, in the presence of mucus, decay or hemorrhages - softer, does not have a clear limitation from neighboring tissue. When cut, it is not difficult to determine its cartilaginous nature;
- upon microscopic examination, the tumor sometimes resembles a chondroma and consists of immature cells with pronounced cellular atypia;
- Often the tumor pattern has the appearance of a microsarcoma, in which areas of cartilage tissue with poorly formed cells containing irregularly shaped chondroblasts can be found [1].
Symptoms and manifestations of pathology
Pain syndrome
Sarcoma of the humerus, or any other, is distinguished by the fact that already at the initial stage of its development it is expressed by a pain syndrome that does not depend in any way on physical activity. Moreover, in a completely relaxed state there is no relief. As the pathological process develops, the intensity and nature of the pain changes. Starting with an intermittent, dull pain, it gradually becomes deep. A clear sign of bone sarcoma is that the condition worsens at night, and taking analgesics does not bring any results.
At a certain point, a swelling of dense consistency forms under the skin in the affected area, has no clear boundaries and is painful when palpated. The skin directly above the swelling becomes hot, and at the same time the subcutaneous veins dilate.
Attention! Pain is not always an indicator of bone cancer, but this circumstance cannot be ignored.
At the next stage of development of bone sarcoma, symptoms appear in the form of impaired functioning of nearby joints. When the disease occurs, a particularly large neoplasm affects functional cells, the bone itself becomes fragile, which is why any injury can result in a fracture. If this does happen, then the development of the tumor accelerates even more.
In addition to the specific symptoms of bone sarcoma, which can be seen in the photo, there are manifestations in the form of:
- increased body temperature;
- sensations preceding vomiting;
- malaise and weakness;
- leukocytosis;
- sometimes the patient develops a fever.
Often, the severity of clinical manifestations of the disease is cyclical in nature, sometimes this leads to misconceptions about the diagnosis. For example, the pain syndrome in the conditions of this disease can either become more intense or decrease. In medical practice, there have been cases where a patient experienced symptoms for more than three months before a correct diagnosis was made. No matter how obvious the manifestations of the disease may be, you should always immediately consult a doctor who will make an accurate diagnosis and prescribe the correct treatment.
General etiology
The causes of sarcomas are varied:
- precancerous diseases (form the basis of the etiology of sarcomas) [2];
- genetic predisposition, some genetic syndromes and hereditary diseases;
- chemical and physical carcinogenesis;
- radiation[9];
- oncogenic viruses (for example, human herpes virus (HHV-8))[10];
- malignancy (malignancy) of benign tumors;
- mechanical damage to tissue (bruise, burn and other injuries);
- foreign bodies (splinters, etc.);
- rapid hormonal growth during puberty. Since sarcoma of the femur occurs mainly in children and adolescents, intensive growth of bone tissue is considered one of the reasons for its occurrence. It has been established that tall boys are more susceptible to the disease[5].
Clinical manifestations
The clinical picture and course depend on the biological characteristics of the original cells and the location of the tumor. For most sarcomas, the first symptom is the appearance of an increasing tumor mass. With bone sarcoma (osteosarcoma, Ewing's sarcoma, etc.), the first sign of the disease is night pain in the area of the affected bone, which is practically not relieved by taking analgesics in standard doses. As a result of tumor growth, neighboring organs and tissues may be involved in the pathological process, which leads to the appearance of corresponding symptoms (for example, when the tumor compresses and/or invades blood vessels, the venous network expands (abundant vascularization); when nerve trunks are damaged, conductive pain occurs along the affected nerves, when the process spreads to the trachea, breathing disturbances are observed, etc.).
Some types of sarcoma, such as parosteal sarcoma of the bone, are characterized by unusually very slow growth and can exist almost asymptomatically for several years. While other types of sarcomas (usually low-grade tumors with high proliferative activity, such as rhabdomyosarcoma), on the contrary, are characterized by rapid (over several months or even weeks) progression, extensive local spread and early metastasis, which usually occurs through the hematogenous route. Some types of sarcomas (for example, liposarcomas) are characterized by simultaneous or sequential appearance in different places of the body, which often makes it difficult to resolve the issue of their metastasis.
Symptoms of sarcoma
The first and most important sign of the disease is pain. Pain sensations occur in the area of the affected area of the bone and are of a constant aching nature. Pain with sarcoma differs from discomfort with injury or inflammation of the joint in that it does not subside at rest and after fixation of the limb. On the contrary, the pain may be worse at night. Also, pain tends to increase and intensifies with palpation of the limb.
If a bone sarcoma develops on the humerus, femur, tibia or fibula, swelling of the limb develops. The damaged arm or leg increases in volume and cannot perform its functions normally. If the leg is affected, lameness occurs.
Later symptoms of the disease:
- the presence of a visible or palpable tumor;
- bone fracture caused by load redistribution due to tumor growth;
- the tissue above the tumor often swells, hyperemia develops, and the temperature in this area may be elevated;
- the veins of the skin over the tumor are dilated;
- general weakening of the body; symptoms of intoxication increase: weakness, nausea, dizziness and headaches, increased body temperature, weight loss;
- A laboratory blood test may reveal anemia due to bone marrow damage.
General methods of diagnosis and treatment
Diagnosis of sarcomas should be based on the use of various techniques, including:
- examination of the patient,
- laboratory tests (histocytological, cytochemical, etc.),
- radiography,
- Ultrasound,
- Doppler angiography,
- Magnetic resonance imaging (MRI),
- Biopsy (open or excisional and closed or incisional),
- Computed tomography (CT),
- Radionucleotide examination (for example, the isomer of the radioisotope technetium-99 - 99Tcm).
Of great importance in diagnosis (especially for choosing adequate treatment) is the determination of the stage of the disease, which takes into account the local spread of the tumor and the presence or absence of distant metastases.
Treatment
The main treatment for sarcomas is surgery[2]. If the removed tumor is successfully located, all body functions are preserved and treatment does not lead to disability. However, very often after tumor removal, malignant growth is observed in the lungs[11].
Additional treatments include chemotherapy and radiation therapy, which are given both before and after surgery[3]. Chemotherapy significantly improves the prognosis for many sarcoma patients, especially those suffering from bone sarcomas (osteosarcomas, Ewing's sarcoma)[3]. For many patients, treatment can be a long and difficult process, lasting about a year[3].
Combination treatment is most effective.
Diagnosis of the disease
The primary methods for diagnosing bone sarcoma are:
- taking anamnesis;
- physical examination;
- X-ray examination.
The patient complains of pain, and there is often a history of trauma. Upon examination, a tumor is identified. X-rays can confirm the presence of bone cancer. More accurate data is provided by computed tomography, which works on the principle of x-rays, only scanning occurs from many sides, resulting in a two- or three-dimensional image. Using CT, the location, size and extent of the sarcoma are assessed. The type of tumor is also preliminarily indicated, which is determined by characteristic features.
Osteolytic osteosarcoma can be distinguished by the presence of a periosteal visor or spur. Bone destruction is visible as a light shadow in place of the bone pattern. Osteoplastic osteosarcoma is characterized by foci of sclerosis at an early stage, bone compaction and osteoporosis at a late stage. Wedge-shaped visors and needle-shaped periostitis are also visible.
Ewing's sarcoma is visible on an x-ray as multiple small foci of destruction. The medullary canal is expanded, and the diaphysis is thickened.
Read here: Pancreatic Oncology
In addition to x-rays of bones, it is necessary to conduct an examination of the chest organs, abdominal cavity and abdominal space, pelvic organs, and skeletal scintigraphy. These procedures are aimed at identifying metastases. Ultrasound is used to check the liver, pancreas, kidneys, and spleen.
Additional tests to diagnose bone sarcoma:
- general blood and urine analysis;
- biochemical blood test, with determination of bilirubin, urea, creatinine, proteins);
- coagulogram;
- determination of blood group and Rh factor;
- ECG.
For differential diagnosis, precise techniques such as MRI and PET can be used.
The decisive analysis will be a biopsy - sampling of tumor material for cytological and histological examination in the laboratory. Based on the biopsy, an accurate diagnosis can be made.
Forecasts
Basically, the prognosis depends on a number of factors: the degree of malignancy, the stage and growth of the tumor, the adequacy and success of treatment of tumors.
Soft tissue sarcomas (liposarcoma, rhabdomyosarcoma) have an unfavorable prognosis, this is primarily due to their tendency to early metastasis. In stage IV soft tissue sarcomas, the 5-year survival rate does not exceed 20%[7]. Factors that improve the survival of patients with soft tissue sarcoma include: age less than 50 years; low grade of sarcoma; pain in the area of the tumor; small size of the tumor and its location on the extremities; absence of metastases[12].
Bone sarcoma: treatment
Can bone sarcoma be cured? Some of the types of this disease are treatable and have good prognoses. But most are still fatal. Early detection of the tumor and complex therapy can extend the survival of patients by 1-5 years or more. Death occurs due to the progression of the disease and the development of metastases. Most often, treatment for bone sarcoma consists of radical surgery to remove the tumor and chemotherapy.
Bone Tumor Surgery
Surgery is the main component of almost any complex for the treatment of bone tumors.
It can be of 2 types:
- Organ-preserving (resection of the bone or its segment, followed by prosthetics).
- Mutilation (amputation, disarticulation).
Doctors, if possible, try to save the limb. Nevertheless, the operation should be as radical as possible. In addition to the tumor, about 5 cm of surrounding healthy tissue is removed. In some cases, this approach leads to rapid relapses of the disease, which requires repeated operations.
Amputations and disarticulations are indicated for widespread tumor spread, bleeding, severe intoxication of the body and pathological fractures with high pain syndrome.
What surgical methods are used for sarcoma? For tumors of the lower jaw, a resection can be performed with cutting out the affected bone or the jaw can be completely removed, and for sarcoma of the tibia, a marginal resection in one block can be performed.
The most common surgical intervention for pelvic tumors is resection of the iliac wing. In this case, the pelvic ring can be preserved and reconstruction will not be needed. More extensive operations require reconstruction, for which autografts or artificial prostheses are used. In advanced cases, when the sacrum is involved in the process, interiliac-abdominal amputation is performed, which involves removing half of the pelvis with a free limb.
It is worth noting that most patients are admitted to the oncology department with large tumors that have already spread greatly. This greatly complicates the possibilities of radical treatment, and sometimes makes it impossible. Another difficulty is associated with sarcomas that are located in hard-to-reach places, for example, in the pelvic bones or spine. It is not always possible to remove them, since there is a high probability of disability for the patient. Surgical treatment for sarcoma of the skull bone is not performed at all.
For Ewing's sarcoma and reticulosarcoma of bone, surgery is rarely performed - in 20% of cases. The reason is low efficiency and high risk of complications. The indication for its implementation is relapse or severe pain that cannot be relieved by conservative methods.
Treatment with chemotherapy
The use of surgical interventions as an independent treatment is justified only for low-grade sarcomas: parossal osteosarcoma, fibrosarcoma, etc. High-grade tumors require a combined approach, including the use of cytostatics - drugs that suppress the growth of sarcomatous cells and lead to their death.
Chemotherapy for bone sarcoma can be preoperative and postoperative. The first is aimed at reducing the size of the tumor and improving the patient's condition. The second is to destroy the remains of the tumor and consolidate the results of the operation. According to statistics, adjuvant chemotherapy can reduce the likelihood of subsequent metastasis by 3.5 times!
If for any reason surgical treatment of bone sarcoma is contraindicated, chemotherapy is used as the main treatment. Chemotherapy for bone sarcoma should primarily consist of several drugs. They are taken in courses (from 3 to 9 or more), orally or through droppers, in certain doses, which are established by an oncologist. Between courses there is a break of 2-3 weeks. The effectiveness of the drugs is assessed based on postoperative examination of the tumor material. If the response was poor, the chemotherapy regimen is changed.
The following medications are used to treat bone sarcomas:
- Adriamycin
- Cisplatin
- Doxorubicin
- Methotrexate
- Cyclophosphamide
- Vincristine
- Sarcazoline
Radiation therapy for bone sarcoma
Irradiation of bone sarcoma is indicated for some types. Ewing's sarcoma is the most sensitive to radiation therapy. Reticulosarcma is similar to it. For them, radiation therapy with prophylactic chemotherapy is the best method. Good results are obtained using a total focal dose of 50-60 Gy. The entire bone containing the tumor is irradiated.
Read here: Is blood cancer transmitted?
The inclusion of radiation therapy in the preoperative period for osteogenic sarcoma can slightly reduce the risk of recurrence. The total focal dose is 30-35 Gy.
Radiation therapy for bone sarcoma in patients with the last stage and multiple metastases helps relieve pain and alleviate the general condition.
Chemotherapy and radiation therapy have their negative consequences. The most common of them are: indigestion, vomiting, nausea, baldness, anemia and weakness, problems with urination, skin reactions. Also, during the treatment period, the immune system is very weak, so there is a high probability of contracting an infection. To combat such consequences, special drugs are prescribed (antiemetics, antibacterials, etc.).
Notes
- ↑ 1234
Handbook of Oncology / edited by prof. B. E. Peterson. - Tashkent: Medicine, 1966. - 500 p. - ↑ 123
Peterson B. E. Oncology (textbook for medical institutes). - M.: Medicine, 1980. - 447 p. - ↑ 1234
Buecker, P (2005). "Sarcoma: A Diagnosis of Patience". ESUN 2 (5). Retrieved 2009-04-15. - Longhi A, Errani C, De Paolis M, Mercuri M, Bacci G (Oct 2006). "Primary bone osteosarcoma in the pediatric age: state of the art." Cancer Treat Rev. 32 (6): 423-36. doi:10.1016/j.ctrv.2006.05.005. PMID 16860938
- ↑ 12
Bone sarcoma: symptoms, causes, treatment. Retrieved April 18, 2013. Archived April 20, 2013. - ^ Darling, J (2007). "A Different View of Sarcoma Statistics". ESUN 4 (6). Retrieved 2012-10-06.
- ↑ 12
Soft tissue sarcomas. Retrieved April 17, 2013. Archived April 20, 2013. - Speech by EESG coordinator AAFedenko at the conference “Man and Medicine”. Retrieved April 17, 2013. Archived April 20, 2013.
- Epidemiology of sarcoma. Per. from English N. D. Firsova (2017).
- Causes of sarcomas. Retrieved April 18, 2013. Archived April 20, 2013.
- Sarcoma and everything you need to know about its diagnosis and treatment. Retrieved April 17, 2013. Archived April 20, 2013.
- SARCOMA. Retrieved April 17, 2013. Archived April 20, 2013.