Description
Urticaria is common: approximately every third person will experience it at least once during their lifetime. In the structure of diseases of allergic origin, urticaria ranks second after bronchial asthma, and in some countries even first. Urticaria is most often observed between the ages of 21 and 60 years, predominantly in women; It is less common in children and the elderly. According to various authors, patients have a burdened allergic heredity.
It is known that the common pathogenetic link of all types of urticaria is an increase in the permeability of microvasculature vessels and the rapid development of edema. The mediators that cause an increase in vascular permeability may be different in each case, but almost all of them relate to mediators of different types of allergic reactions. Similar mediators are also involved in the development of pseudoallergic reactions. In this regard, two pathogenetic forms of urticaria can be distinguished - allergic and pseudoallergic. Allergic urticaria is caused by allergens; it has an immune mechanism.
Urticaria is pseudoallergic, the mediators of which are formed without the participation of the immune mechanism.
In allergic urticaria, the allergens most often are drugs, foods, and insect allergens. In pseudoallergic urticaria, the active factors are drugs (antibiotics, radiocontrast agents, etc.), serums, immunoglobulins, bacterial polysaccharides, food products and the xenobiotics they contain, physical factors (cold, solar radiation, etc.). The leading pathogenetic link in the development of this form of urticaria is diseases of the digestive system and, first of all, dysfunction of the hepatobiliary system.
Clinical picture
Acute urticaria begins suddenly with severe itching of the skin of various parts of the body, sometimes its entire surface. It may be accompanied by malaise, headache, and often a rise in body temperature to 38 - 39 0C. Soon, hyperemic rashes appear on the itchy areas, protruding above the surface of the skin - blisters. As the swelling increases, the capillaries are compressed and the blister turns pale. In the center of the edema, a vesicle may form with detachment of the epidermis.
The exudate can become hemorrhagic in nature, and later pigment spots are formed as a result of the breakdown of red blood cells. Elements of the rash can have different sizes - from small (the size of a pinhead) to gigantic. They are located separately or merge, forming bizarre figures with scalloped edges. The rash appears and disappears, remaining in one place for several hours and then reappearing in another area. The duration of the acute period is from several hours to several days, after which they speak of the subacute form of urticaria. If the total duration of urticaria exceeds 3 weeks, the disease becomes chronic.
Chronic recurrent urticaria occurs in waves, sometimes over a very long time (up to 20–30 years) with periods of remission. This form is accompanied by particularly painful itching. Patients scratch their skin until it bleeds. As a result of scratch infection, pustules and other elements appear.
Classification, types of urticaria and pathogenesis
A blister is a local swelling of the dermis, usually characterized by itching, limited swelling of the skin, and hyperemia. The blister completely resolves within a relatively short time.
In addition to dividing urticaria into acute and chronic, there is a division into types depending on the factors that provoke exacerbation. The same patient may experience different forms of urticaria at the same time.
In addition, a number of conditions are described that at one time were classified as urticaria, but are not such, or contain urticaria/angioedema as one of the symptoms of the clinical picture:
- Urticaria pigmentosa (mastocytosis) is a disease caused by the accumulation and proliferation of mast cells in tissues.
- Polymorphic skin rashes, including urticarial ones, are characteristic.
- Urticarial vasculitis - vasculitis with skin rashes - nodules and blisters, angioedema. After resolution of the elements, hyperpigmentation may be observed.
- Nonhistaminergic angioedema, such as hereditary angioedema, often associated with defects in the complement or kinin system.
- Exercise-induced anaphylaxis/urticaria.
- Cryopyrin-associated periodic syndrome (in the clinic there is an urticarial rash, fever, arthralgia or arthritis, increased fatigue and headaches. Includes familial cold autoinflammatory syndrome (Muckle-Wells syndrome (with the development of sensorineural hearing loss and renal amyloidosis) and infantile multisystem inflammatory disease .
- Schnitzler syndrome is a chronic urticaria with monoclonal IgM gammopathy.
- Gleich syndrome is episodic angioedema with eosinophilia.
- Wells syndrome is a granulomatous dermatitis with eosinophilia.
Causes of urticaria
To cure urticaria, it is necessary to identify the cause that caused the disease. It is possible that the cause of hives could be some food, then they should be excluded from the diet. Hives can occur due to severe stress. This disease is treated with special ointments that must be prescribed by the attending physician.
The problem is encountered by those who want to get rid of hives using conventional cosmetics, assuming that this is a common skin irritation. In fact, the real cause of hives is allergies. An allergic reaction can be caused by foods, medications, chemicals, pollen, as well as the influence of heat or cold, and also cosmetics. For this reason, the desire to disguise hives with foundation can aggravate the situation.
Diet
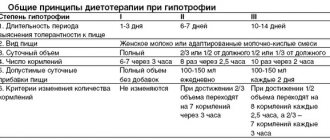
A hypoallergenic diet for urticaria consists of several provisions:
- Drinking regime. You need to drink at least 2 liters of water per day.
- For allergies, during the first 24 hours the diet is based on low-fat kefir.
- Gradually, you can start eating dietary chicken and potatoes, pre-soaked for a day.
- You can gradually introduce green vegetables and fruits. Also soak the porridge for a day before cooking. Steam food. Take with water, exclude drinks.
- On day 3 you can eat pears, bananas, beef.
- Until the cause of hives is determined, exclude chocolate, eggs, nuts, coffee, tea, smoked and fried foods, sweets, honey, spices and seasonings, and alcohol.
- Minimum: carrots, beets, fish, milk.
- The main rule is to introduce the product gradually, in small portions; if any reactions develop, immediately write it down in your diary and tell your doctor.
Urticaria itself is not a dangerous disease, but with high sensitization, angioedema can occur. If the laryngeal tissues swell, suffocation is possible. The reaction is rapid and can be fatal. Therefore, it is important to understand the causes of urticaria allergies and prevent its occurrence.
Symptoms of the disease Urticaria
Clinically, the following types of urticaria are distinguished:
- acute urticaria (this also includes acute limited angioedema);
- chronic recurrent;
- persistent papular chronic urticaria.
Acute urticaria
This disease appears suddenly and is characterized by the appearance of a very itchy urticarial rash with elements of different sizes. Blisters are more often round in shape and somewhat less often irregularly elongated. The rashes rise above the skin level, in the center with a matte tint, and along the periphery you can see a fuzzy pink border.
Blisters can merge into fairly large areas. In such cases, the general condition of the body is disturbed in the form of increased body temperature with chills (called “nettle fever”), gastrointestinal disorders, and general malaise. The locations of the loose elements are mainly the torso, arms, and buttocks. In addition, rashes can appear on the mucous membranes of the lips, soft palate, tongue, nasopharynx, and larynx, often making breathing and swallowing difficult.
The rash in acute urticaria does not last long, usually within 1-2 hours. In total, this form of the disease lasts several days. Most often, acute urticaria is a form of drug or food allergy, as a response to the administration of therapeutic serums, vaccines, blood transfusions, etc. There is also an atypical form of acute urticaria, which is a consequence of mechanical irritation of the skin. This can usually be when dermographism is detected. The blisters in this form of acute urticaria have a linear shape and differ from ordinary urticaria in the absence of itching.
Acute limited angioedema
This disease has other names: giant urticaria, angioedema. It is clinically manifested by the sudden development of limited swelling of the skin or mucous membrane and subcutaneous fatty tissue, for example lips, cheeks, eyelids, genitals, etc. The skin in such affected areas is densely elastic to the touch, white, less often pink. Patients may complain of burning and itching, but more often there are no subjective sensations. Usually after a few hours or 1-2 days the swelling subsides. Relapse is possible. Sometimes Quincke's edema is combined with ordinary urticaria. If swelling develops in the larynx, then stenosis and asphyxia are possible. Swelling located in the orbital area can cause deviation of the eyeball in the medial direction and decreased visual acuity.
Chronic recurrent urticaria
This form of the disease is a consequence of long-term sensitization, which is caused by the presence of foci of chronic infections in the body, such as tonsillitis, adnexitis, caries, etc., as well as dysfunction of the gastrointestinal tract, liver, etc. Chronic urticaria is characterized by a paroxysmal course and differs from acute urticaria with less profuse rashes. The rash appears on various areas of the skin. The appearance of a rash may be accompanied by general weakness, fever, headache, joint pain, and if the mucous membranes of the gastrointestinal tract are affected, nausea, vomiting and diarrhea. Patients complain of painful itching, which leads to neurotic disorders and insomnia. A blood test reveals eosinophilia and thrombocytopenia.
Persistent papular urticaria
If persistent, long-lasting urticarial rashes progress to the papules stage, then persistent papular urticaria develops. In this case, hyperkeratosis and acanthosis join the phenomena of persistent limited swelling of cellular infiltration in the dermis. The nodules are located mainly on the extensor surfaces of the limbs and are red-brown in color. Women get sick more often.
Some authors consider this form of urticaria as a type of prurigo.
Solar urticaria
It is a type of photodermatosis that develops in patients with liver diseases with increased sensitization to ultraviolet rays in people with impaired porphyrin metabolism. It is observed mainly in women. With this disease, urticarial rashes appear on open areas of the skin (face, upper extremities, etc.). Seasonality is characteristic (spring, summer), since at these times of the year the activity of ultraviolet rays is especially high. Staying in the sun for such patients for a long time can lead to a general reaction of the body in the form of respiratory failure, cardiac activity, and even shock.
Diagnosis of urticaria
If hives appear suddenly, disappear quickly and do not recur, then medical examination is not required, as the cause is usually obvious. But it is necessary if angioedema or urticaria recurs for no apparent reason.
Allergic contact dermatitis
Clinical manifestations
Allergic contact dermatitis develops in those working with drugs at the initial stage in the form of monovalent sensitization. In areas of contact with the allergen, areas of hyperemia with papules or blisters accompanied by itching are observed. At the initial stage, the allergen concentration is important for the occurrence of contact allergic dermatitis; with repeated contacts, the disease manifests itself at minimal concentrations.
Initially, changes occur in the form of dermatitis on open areas of the skin (hands, neck, face) or in the form of allergic rhinitis in cases of exposure to medicinal aerosols. Subsequently, allergic dermatitis or rhinitis can transform into systemic manifestations - toxicdermia.
Treatment
1. Elimination of contact with the allergen, in cases of occupational disease - employment without contact with medicinal substances. 2. Treatment on an outpatient basis with second-generation antihistamines - Claritin or Ebastine - 1 table. (10 mg) once daily. The duration of treatment depends on the duration of the disease. 3. Local glucocorticoid Elokom in the form of an ointment or gel - lubrication once a day in places of greatest inflammation of the skin. 4. Hypoallergenic diet.
Treatment of urticaria
An obligatory component of the treatment of urticaria is adherence to a diet and a special lifestyle (more details in the section Features of nutrition and lifestyle with urticaria). It should be noted that for urticaria, a number of medications that may be prescribed to treat concomitant diseases of a patient with urticaria are prohibited. These drugs include: aspirin and its derivatives, codeine, ACE inhibitors (enap, enam, capoten, etc.). If you suffer or have suffered from urticaria, you should definitely warn your doctor about this so that he does not prescribe you medications that can provoke an exacerbation.
Traditionally, treatment for urticaria begins with antihistamines. It is preferable to use 3rd generation drugs: Telfast, Zyrtec, Erius, etc. Sometimes (with chronic urticaria) long-term medication is required, up to three months or more.
Anti-leukotriene drugs, for example, Singulair, are used to treat urticaria with good effect. The drug is available in dosages of 5 (for children) and 10 milligrams. The course of treatment is from 10 days to 1 month. Sometimes longer. Singulair has a very good effect on cold urticaria.
In severe forms of urticaria that are resistant to therapy, it is possible to prescribe corticosteroids in doses of up to 1 mg per kg of body weight for 5-7 days until remission is achieved with a gradual dose reduction. Drugs: prednisolone, metipred, etc. This treatment may be associated with a large number of side effects, and therefore can only be carried out as prescribed and under the supervision of a physician.
Urticaria is often observed in patients under stress, in patients with increased anxiety, etc. In addition, prolonged itching constantly bothers patients, figuratively speaking, “inflating” the nervous system, as a result of which the disease progresses. In these cases, anxiolytics can be used, for example, atarax, bellataminal, paroxetine, etc.
In chronic forms of urticaria, plasmapheresis, the so-called hardware blood purification, can be used. For many forms of urticaria, the administration of histoglobulin is effective. Course from 5 to 15 injections.
If skin lesions do not go away for a long time, ointments and creams containing corticosteroids are used to remove them. Preference is given to the latest generation of drugs that do not contain halogens (fluorine, chlorine), for example, Advantan, Lokoid. Duration of use is no more than 10 days in a row.
The above measures for the treatment of urticaria are adjusted depending on the results of the examination. For example, they normalize the functioning of the gastrointestinal tract, “etch” parasites, etc.
Evaluation of urticaria control[ | ]
The Urticaria Control Test is used to assess disease control over the past 4 weeks in patients with chronic spontaneous and induced urticaria. It is required to answer 4 questions regarding control of symptoms of the disease, impact on quality of life, effectiveness of treatment, and overall control of the disease.
Each answer to a question is scored on a scale from 0 to 4. The maximum score for answering questions is 16, demonstrating complete control of the disease. The threshold value is 12 points. UCT ≤ 11 points indicates uncontrolled chronic urticaria[18].
Urticaria, treatment with folk remedies
Elimination of the disease using traditional medicine is possible . Oddly enough, nettle is considered a raw material for the effective treatment of this disease.
The skin deformations that urticaria causes and how to treat them at home using folk remedies have long been known to those who have already encountered this disease.
They recommend doing:
- Drink with a string. It is brewed in the same way as tea, pouring boiling water over it and waiting 20 minutes. They should replace all their usual daily drinks.
- A tincture that is very easy to prepare from nettle. You need to pour a tablespoon of dried flowers of this plant into 200 ml. boiling water Then cover the container with the medicine with a cloth, leave for 30 minutes, and then strain. You should drink half a glass several times a day (4-5) .
- Lotions with nettles. To make the desired composition for them, you need to put 30 grams in a saucepan. leaves of the plant, pour two glasses of water and wait until it boils. Then reduce the heat, wait 3 minutes, remove the dishes and leave to cool for 60 minutes. Next, strain everything. Such lotions can be applied several times a day.
- Water showers are often recommended to relieve itching. Based on the causes of the disease and accompanying symptoms, it can be cold in one case, and hot in another.
- Mint infusion. It is valued for its remarkable calming properties, as well as for its beneficial effect on the functioning of the digestive tract. To make it, you need to brew mint leaves with boiling water and drink a sip several times a day.
Numerous tips from folk practice can tell you how to treat urticaria at home.
The most common recipes that are perfect for local therapy:
- Ointment for hives on the skin (it can quickly eliminate the signs of the disease. To prepare it, you should finely chop a head of garlic and pour two cups of boiling water into it. Then you need to boil everything until half the liquid has evaporated. Next, remove the solution from the heat, add mix a glass of oil (vegetable or olive) and a small amount of beeswax into it. Apply this ointment to clean, affected skin several times a day. Store it in the refrigerator).
- Soothing paste for irritated skin (you need to mix 3 tablespoons of soda, a large spoon of water and the same amount of vegetable oil. All ingredients are mixed and applied to irritated areas repeatedly, all day).
Video
Notes[ | ]
- Disease ontology database (English) - 2020.
- ↑ 123
Monarch Disease Ontology release 2018-06-29sonu - 2018-06-29 - 2018. - ↑ 12
Urticaria // Great Medical Encyclopedia, T. 11. - 3rd ed. - M.: "Soviet Encyclopedia", 1979. - P. 491-493. - ↑ 12345
Federal clinical guidelines of the RAAKI for the diagnosis and treatment of urticaria. Approved by the Presidium of RAACI on December 25, 2015. — Russian Allergological Journal, 2020 — No. 1: 37-45 (Last access date: 11/19/2018) - ↑ 12345
Federal clinical guidelines. Dermatovenerology 2020. Skin diseases. Sexually transmitted infections. — 5th ed. reworked and additional — M: Business Express, 2020. — 768 p. (Last access date: 11/19/2018) - ↑ 1 2 3 4 5 6 7 8 9 10 Zuberbier T, Aberer W, Asero R, Abdul Latiff AH, Baker D at all.
The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. - Allergy, 2018 Jul - 73(7):1393-1414. - doi: 10.1111/all.13397. (Last access date: 11/19/2018) - Zitelli, Kristine B., and Kelly M. Cordoro.
Evidence-Based Evaluation and Management of Chronic Urticaria in Children. — Pediatric dermatology 28.6, 2011—629−639 (Last access date: 11/19/2018) - Maurer M, Weller K, Bindslev-Jensen C, Giménez-Arnau A, Bousquet PJ at all.
Unmet clinical needs in chronic spontaneous urticaria. A GA²LEN task force report. - Allergy, 2011 Mar - 66(3):317-30. - doi: 10.1111/j.1398-9995.2010.02496.x. (Last access date: 11/19/2018) - Silpa-archa N, Kulthanan K, Pinkaew S.
Physical urticaria: prevalence, type and natural course in a tropical country. - J Eur Acad Dermatol Venereol, 2011 Oct - 25(10):1194-9. - doi: 10.1111/j.1468-3083.2010.03951.x. (Last access date: 11/19/2018) - Maurer M, Abuzakouk M, Bérard F, Canonica W, Oude Elberink H at all.
The burden of chronic spontaneous urticaria is substantial: Real-world evidence from ASSURE-CSU. - Allergy, 2020 Dec - 72(12):2005-2016. - doi: 10.1111/all.13209. (Last access date: 11/19/2018) - O'Donnell BF, Lawlor F, Simpson J, Morgan M, Greaves MW.
The impact of chronic urticaria on the quality of life. - Br J Dermatol, 1997 Feb - 136(2):197-201. — PMID: 9068731 (Last access date: 11/19/2018) - Pavel Kolkhir, Galina Balakirski, Hans F. Merk, Olga Olisova, Marcus Maurer.
Chronic spontaneous urticaria and internal parasites – a systematic review (English) // Allergy. — 2015-12-01. — P. n/an/a. — ISSN 1398-9995. - doi:10.1111/all.12818. - ↑ 1 2 Kaplan AP, Greaves M.
Pathogenesis of chronic urticaria. - Clin Exp Allergy, 2009 Jun - 39(6):777-87. - doi:10.1111/j.1365-2222.2009.03256.x. (Last access date: 11/19/2018) - Sabine Altrichter, Hans-Jürgen Peter, Dina Pisarevskaja, Martin Metz, Peter Martus and Marcus Maurer.
IgE Mediated Autoallergy against Thyroid Peroxidase – A Novel Pathomechanism of Chronic Spontaneous Urticaria? PLoS One, 2011 - 6(4): e14794. — DOI:10.1371/journal.pone.0014794 (Last access date: 11/19/2018) - Kaplan, Allen P., Anna Maria Giménez‐Arnau, and Sarbjit S. Saini.
Mechanisms of action that contribute to the efficacy of omalizumab in chronic spontaneous urticaria. — Allergy 72.4, 2020 — 519-533. (Last access date: 11/19/2018) - Schmetzer, Oliver, et al.
IL-24 is a common and specific autoantigen of IgE in patients with chronic spontaneous urticaria. — Journal of Allergy and Clinical Immunology 142.3, 2020 — 876-882. (Last access date: 11/26/2018) - Stone KD, Prussin C, Metcalfe DD.
IgE, mast cells, basophils, and eosinophils. - J Allergy Clin Immunol, 2010 Feb - 125(2 Suppl 2):S73-80. - doi: 10.1016/j.jaci.2009.11.017. (Last access date: 11/19/2018) - Weller, Karsten, et al.
Development and validation of the Urticaria Control Test: a patient-reported outcome instrument for assessing urticaria control. - Journal of Allergy and Clinical Immunology 133.5, 2014 - 1365-1372. (Last access date: 11/23/2018) - ↑ 1 2 Danilycheva I.V., Shulzhenko A.E.
Severe urticaria - Russian Journal of Allergology, 2020. - T. 14., no. 3. – 64-75 p. (Last access date: 11/19/2018) - Ministry of Health of Russia: Standard of emergency medical care for angioedema, urticaria. Order No. 1430n dated December 24, 2012 // garant.ru, //consultant.ru (Last access date: 11/19/2018)
- Kozel MM, Mekkes JR, Bossuyt PM, Bos JD.
Natural course of physical and chronic urticaria and angioedema in 220 patients. - J Am Acad Dermatol, 2001 - 45(3):387. (Last access date: 11/19/2018) - How to prescribe antihistamines for chronic idiopathic urticaria: desloratadine daily vs PRN and quality of life. Grob JJ, Auquier P, Dreyfus I, Ortonne JP Allergy. 2009 Apr;64(4):605-12. Epub 2008 Dec 30.
- Antihistamines in the treatment of chronic urticaria. Jáuregui I, Ferrer M, Montoro J, Dávila I, Bartra J, del Cuvillo A, Mullol J, Sastre J, Valero A J. Investig Allergol Clin Immunol. 2007;17 Suppl 2:41.
- Effect of the H2-antagonist cimetidine on the pharmacokinetics and pharmacodynamics of the H1-antagonists hydroxyzine and cetirizine in patients with chronic urticaria. Simons FE, Sussman GL, Simons K. J Allergy Clin Immunol. 1995 Mar;95(3):685-93.
- ↑ 12
Registration certificate State Register of Medicines - Saini SS, Bindslev-Jensen C, Maurer M, Grob JJ, Bülbül Baskan E at all.
Efficacy and safety of omalizumab in patients with chronic idiopathic/spontaneous urticaria who remain symptomatic on H1 antihistamines: a randomized, placebo-controlled study. - J Invest Dermatol, 2020 Jan - 135(1):67-75. - doi: 10.1038/jid.2014.306. (Last access date: 11/19/2018) - Marcus Maurer, MD, Karin Rosén, MD, Ph.D., Hsin-Ju Hsieh, Ph.D., Sarbjit Saini, MD, Clive Grattan at all.
Omalizumab for the Treatment of Chronic Idiopathic or Spontaneous Urticaria. - N Engl J Med 2013 - 368:924-935. — DOI: 10.1056/NEJMoa1215372 (Last access date: 11/19/2018) - Kaplan A1, Ledford D, Ashby M, Canvin J, Zazzali JL at all.
Omalizumab in patients with symptomatic chronic idiopathic/spontaneous urticaria despite standard combination therapy. - J Allergy Clin Immunol, 2013 Jul - 132(1):101-9. - doi: 10.1016/j.jaci.2013.05.013. (Last access date: 11/19/2018) - Casale TB, Bernstein JA, Maurer M, Saini SS, Trzaskoma B at all.
Similar Efficacy with Omalizumab in Chronic Idiopathic/Spontaneous Urticaria Despite Different Background Therapy. - J Allergy Clin Immunol Pract, 2020 Sep-Oct - 3(5):743-50.e1. - doi:10.1016/j.jaip.2015.04.015. (Last access date: 11/19/2018) - Schäcke H, Döcke WD, Asadullah K.
Mechanisms involved in the side effects of glucocorticoids. - Pharmacology & Therapeutics, 01 Oct 2002, 96(1):23-43. — DOI: 10.1016/S0163-7258(02)00297-8 (Last access date: 11/19/2018) - Influence of initial treatment modality on long-term control of chronic idiopathic urticaria. Kim S, Baek S, Shin B, Yoon SY, Park SY, Lee T, Lee YS, Bae YJ, Kwon HS, Cho YS, Moon HB, Kim TB. PLoS One. 2013;8(7): e69345. Epub 2013 Jul 23
- The leukotriene receptor antagonist montelukast in the treatment of chronic idiopathic urticaria: a single-blind, placebo-controlled, crossover clinical study. AU Erbagci Z SO J Allergy Clin Immunol. 2002;110(3):484.
- Efficacy of leukotriene receptor antagonist in chronic urticaria. A double-blind, placebo-controlled comparison of treatment with montelukast and cetirizine in patients with chronic urticaria with intolerance to food additive and/or acetylsalicylic acid. Pacor ML, Di Lorenzo G, Corrocher R. Clin Exp Allergy. 2001;31(10):1607.
- Boehm I et al. Urticaria treated with dapsone. Allergy. 1999 Jul;54(7):765-6
- What the first 10,000 patients with chronic urticaria have taught me: a personal journey. Kaplan AP. J Allergy Clin Immunol. 2009;123(3):713.
- Treatment of refractory chronic urticaria with sirolimus. Morgan M. Arch Dermatol. 2009;145(6):637.
- Treatment of severe chronic idiopathic urticaria with oral mycophenolate mofetil in patients not responding to antihistamines and/or corticosteroids. AU Shahar E, Bergman R, Guttman-Yassky E, Pollack S SO Int J Dermatol. 2006;45(10):1224.