Aseptic wound
– this concept is not so much microbiological as clinical. It means that under these conditions the risk of developing a surgical infection is minimal.
Microbially contaminated or contaminated wound
– this is a condition when microorganisms have entered the wound; general and local defense mechanisms are able to restrain them at the stage of the incubation process and there are no clinical signs of an infectious process in the wound.
It is customary to distinguish between primary
and
secondary microbial contamination of a wound
. Primary contamination occurs at the time of injury and is typical for traumatic and gunshot wounds. Secondary wound contamination is usually associated with violation of aseptic rules during dressing changes and is often a manifestation of nosocomial infection.
Infected wound
– this is a wound in which the development of an infectious process occurs, caused by an imbalance between the microbes that have entered the wound and the body’s defenses, which is manifested by clinical symptoms of inflammation. In this case, microbes begin to multiply deep into viable tissues in the lymphatic and blood ducts.
Clinical picture of wounds
consists of a number of clinical symptoms, the main of which are:
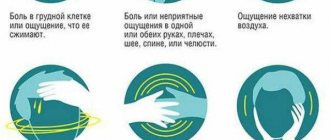
Pain.
Bleeding.
Hiatus.
4. Local and general functional disorders
.
Pain
at the time of injury is determined by damage to receptors and nerve trunks, its intensity depends on the location and type of wound, as well as on the condition of the victim.
Throbbing pain that appears in the wound area some time after the injury characterizes the addition of an infectious process in the wound.
Bleeding
depends on the nature and diameter of the vessel damaged during injury. The most intense and dangerous bleeding is from the cavities of the heart and large arterial and venous trunks.
Hiatus
- divergence of the edges of the wound, associated with the elastic properties of the skin, more pronounced in the wound located perpendicular to the direction of the elastic fibers of the skin (Langer's lines), called skin ridges, muscle and fascial fibers.
First aid for injuries:
$ stopping bleeding in any possible way (pressing the vessel, applying a tourniquet, pressure bandage);
$ protection of the wound from contamination and infection: wound treatment should be carried out with clean, preferably disinfected hands;
$ before applying a bandage, it is necessary to remove dirt, soil, and scraps of clothing from the surface of the wound and adjacent areas of skin with tweezers, a piece of gauze or cotton wool. After this, in the presence of disinfectants (Sol. Peroxydumhydrochloridum - 3% solution; Sol. Furacillinum 1:5000 - 500.0; Sol. Iodispirituosa 5%), it is necessary to widely treat the skin around the wound 2 - 3 times. This prevents infection of the wound from the surrounding skin after applying a bandage; (toilet wound)
$ Do not allow cauterizing antiseptic substances to get into the wound (burn), as they can cause cell death - a sharp increase in pain;
$ Applying an aseptic dressing
, you should not touch with your hands those layers of gauze that will be in direct contact with the wound;
$ If there are small foreign bodies in the wound (shards of glass, metal), remove carefully using tweezers or a clamp;
$ Foreign bodies from large and deep wounds can only be removed by a doctor during primary surgical treatment;
$ Do not wash or dry the wound before applying a bandage. To fix the bandage, you can use adhesive plaster, cleol, mesh-tubular bandages;
$ The wound should not be covered with powders, ointment should not be applied to it, cotton wool should not be applied directly to the wound surface - all this contributes to the development of infection in the wound;
$ Sometimes internal organs (brain, intestine, lung) may be present to the wound. When treating such a wound, the prolapsed organs must not be immersed deep into the wound; a bandage must be applied over the prolapsed organs;
$ Apply analgesics (pain relief).
$ Ensuring complete rest of the injured area through proper immobilization and transportation;
$ Delivery to a medical facility, where in addition to treatment and prevention of tetanus, they are carried out.
A simple wound is not so terrible - many people think so. But if not handled well, it can quickly become a serious problem. Here's how to identify the signs of a developing infection so you can get rid of it before it causes real trouble.
Do you use soap to treat microtraumas?
Surprised to see soap on this list? This is just one common health product that could be harmful to you and your family. Regular hand soap can sometimes irritate the skin, which can slow down the healing process and, in turn, lead to infection of the wound. Of course, each person reacts differently to different cleansers, all this is purely individual. But why take the risk and use soap to treat microtraumas? It is best to avoid using harsh ingredients, namely soap, and use soft moisturizing gels and ointments. They are much more useful than soap.
Main types of complications from wounds and their prevention
1The main types of complications that can occur during injury are bleeding, infection, intoxication, pneumothorax, hemothorax, and traumatic shock.
One of the most common and dangerous types of complications is bleeding. Blood makes up about 7-8% of body weight, i.e. 5.2 kg if the mass is 65 kg. When bleeding, loss of 10% of blood is acceptable, 30% is dangerous, 50% is fatal. During minor bleeding, blood clotting begins after 3 minutes and ends after 8 minutes.
Bleeding to the flow of blood from damaged blood vessels, which can be primary (occurs immediately after the injury) or secondary (appears some time after the injury). Depending on the type of damaged vessels, arterial, venous, capillary and parenchymal bleeding are distinguished.
Arterial bleeding is the most dangerous because it occurs when the arteries are damaged; After all, a significant amount of blood can leak out in a short time; the loss of 2 liters of it can already lead to death. A sign of arterial bleeding is the bright red color of the blood, leakage in a pulsating stream or fountain.
Venous bleeding is also dangerous . Its characteristic feature is a darker color of the blood, the absence of a pulsating stream or fountain. Often these two types of bleeding occur in places where major blood vessels are damaged, located close to the surface of the body.
Capillary bleeding is a consequence of damage to small blood vessels (capillaries) of the skin, subcutaneous tissue or muscles. The entire surface of the wound bleeds.
Parenchymal bleeding - occurs in case of damage to internal organs (liver, kidneys, lungs) and is always life-threatening. Sometimes it occurs with closed injuries of internal organs and is difficult to determine.
Depending on the location of the bleeding, external and internal bleeding are distinguished. During external bleeding, blood flows through wounds in the skin and mucous membranes onto the surface of the body. During internal bleeding, or hemorrhage, blood flows into the tissues of organs or cavities. Pouring into the tissues, the blood saturates them, forming a swelling called infiltrate
, or bruise.
If the blood saturates the tissues unevenly and as a result they diverge, forming a blood-filled cavity, a hematoma
.
First aid for bleeding
Depending on the type of bleeding and the available means to temporarily or permanently stop the bleeding.
Temporary stoppage of bleeding aims to prevent life-threatening blood loss, gain time for transporting the patient and preparing him for surgery. This can be done in several ways:
• raising the injured limb upward;
• applying a pressure bandage;
• maximum flexion in the joints of the injured limb;
• pressing the vessel with a finger above the injury site;
• applying a tourniquet or twist.
The fastest way to temporarily stop arterial bleeding is to press the vessel with your finger. It is used for damaged arteries. The arteries are pressed with fingers against adjacent bones in places where they pass close to the surface of the body. After digital pressure of the arteries, you need to apply a tourniquet (where possible) and a sterile bandage. In case of a head injury with damage to the carotid artery, apply a tight bandage, under which a strong cushion made of bandage and gauze is placed.
A rubber tourniquet is the best way to stop arterial bleeding. It is applied to the thigh, lower leg, shoulder or forearm above the wound site, but not far from the wound itself, on clothing or a layer of bandages or napkins so as not to pinch the skin, with such force as to stop the bleeding, but not to injure the nerve trunks of the limbs. Therefore, tightening is stopped as soon as the cessation of blood flow is observed. If the tourniquet is not applied tightly enough, arterial bleeding may even increase, since the blood pressure in the arteries increases due to the cessation of blood flow through the veins. The cessation of blood supply can be monitored by the absence of a pulse in the peripheral vessels.
Remember that the tourniquet can be applied for no more than 2 hours, but this is the limit. Of course, the tourniquet is kept for no more than 1.5 hours in summer and 1 hour in winter. Without blood supply, the cells of the body's tissues die quite quickly, so be sure to place a note under the tourniquet indicating the time of its application. Tighten the limb with a tourniquet and cover it warmly, especially in winter. The use of anti-shock measures is recommended.
If for some reason the victim was not taken to a medical facility and did not undergo surgical treatment of the wound within 1.5 hours, finger pressure should be applied to the artery and the tourniquet should be loosened for 5-10 minutes to avoid tissue necrosis. Then you need to apply the tourniquet again, but this time above the previous place. This procedure must be performed every 40 minutes until the patient is delivered to the hospital. In this case, each time you need to make a corresponding note in the note.
In the absence of a tourniquet, use twists made from rope, belt or twisted napkin. In this case, care should be taken, since such agents are less elastic and can quickly lead to injury not only to nerve trunks, but also to tissues and muscles.
Maximum flexion of the limb at the joint can also help temporarily stop bleeding. In this case, the limb is securely fixed in a position in which there is less bleeding.
Temporary stoppage of external venous and capillary bleeding is performed using tight bandages. The wound is covered with a napkin or a bandage rolled up in 5-6 layers, absorbent cotton is placed on top and bandaged firmly. To reduce bleeding, it is advisable to raise the damaged part of the body relative to the position of the body. Bleeding from veins with varicose veins in the legs can be especially dangerous. Such veins can burst, causing significant damage. Help should be provided in the same way as for any venous bleeding, but with extreme caution.
Blood loss affects people in different ways. Elderly people and children are most sensitive to it. Losing 300-400 ml of blood can be fatal for them. With significant blood loss, acute anemia develops. In these cases, the person complains of increasing weakness, dizziness, tinnitus, thirst, nausea, and darkening of the eyes. The person may lose consciousness. Convulsions appear. In such cases, it is advisable to place the patient on a flat surface to prevent bleeding of the brain, and free the neck and chest from clothing.
In case of loss of consciousness, a “self-transfusion” of blood can be done, which consists of alternately raising the upper and lower extremities. This helps in better blood flow to vital organs. If the victim is conscious and does not have abdominal injuries, he must be given hot tea or just water. However, the main method of treating acute anemia is an urgent transfusion of donor blood, so the victim must be taken to a medical facility as quickly as possible.
Bleeding into the chest cavity occurs during blows to the chest, rib fractures, due to damage to blood vessels and filling of one or both pleural cavities with blood. This can cause compression of the lungs, which in turn makes breathing difficult and even stops. Symptoms include pale complexion, shortness of breath, rapid pulse. Help consists of placing the victim's body in a semi-sitting position and applying an ice pack to the chest. Of course, the victim must be hospitalized immediately.
Bleeding into the peritoneum occurs more often due to rupture of the liver or spleen. As with bleeding into the chest cavity, the victim's skin becomes pale, cold and clammy, and the pulse becomes weak. The person experiences thirst, severe pain, and may lose consciousness. The patient should be placed on his back, with an ice pack placed on his stomach. Do not feed the victim or give him anything to drink. You can only wet your lips.
1
Neglecting bandages
If you think it's a good idea to let your skin breathe after initially treating any microtrauma, think again. By not covering the wound with a bandage, you expose the skin to infection. New cells must migrate to the appropriate areas for the wound to heal faster. By covering it with a bandage, you make this process easier and faster. The best way to help prevent infection from developing is to apply an ointment to the wound, which you should always have in your home. If you haven't visited a doctor, then at least keep Vaseline in your medicine cabinet. As you know, it prevents the wound from drying out and scabs forming, and accordingly, it heals faster.
Redness and swelling around the wound
It's normal for the skin around a wound or scratch to look a little different. Redness, swelling and even a small bruise appear. The main thing is not to confuse this with an accumulation of pus. You should only panic if these symptoms worsen and the wound does not heal. For example, redness and slight swelling around a cut or scrape are often signs of healing. But when this color does not disappear for a long time or the swelling increases, this indicates that the process of infection of the wound has begun. Do not delay, consult a doctor as soon as possible to avoid dire consequences.
Complications of bite wounds
More than 150 different diseases are transmitted from animals to humans. The transmission of diseases such as rabies, cat scratch disease (benign lymphoreticulosis), sodoku (“rat bite disease”), tularimia, and leptospirosis has been documented. brucellosis, tetanus and others. Hepatitis, tuberculosis, syphilis and other diseases are transmitted through human bites. Infectious complications can be caused by almost any type of bacteria, viruses, spirochetes, and fungi.
We must not forget that an animal attack itself is a severe mental trauma, which is especially dangerous for a child or a person with concomitant pathology.
Bite wounds are characterized by infection with the microflora of the oral cavity of an animal or person. They become contaminated with scraps of clothing, microorganisms from the surface of the skin and from the environment.
Anaerobic microorganisms make up the absolute majority of the normal microflora of the oral cavity of humans and animals; the ratio of aerobes to anaerobes is 1:10, 1:100.
According to many authors, the release of anaerobes beyond their natural habitats is the cause of the occurrence of mixed aerobic-anaerobic infections in places of animal or human bites, as well as on the hand after a blow to the teeth.
When studying the microbial landscape of wounds, anaerobic non-clostridial bacteria are found in 30-95% of cases. Under certain conditions, these pathogens become the cause of the development of one of the most dangerous surgical diseases - anaerobic non-clostridial soft tissue infection (ANIMT). The presence of anaerobic-aerobic associations in the wound leads to characteristic clinical manifestations of infection and requires special surgical tactics and rational antibiotic therapy.
Unfortunately, we did not find specific data on the frequency of detection of anaerobes in bite wounds and on the frequency of development of AIIMT in the literature.
Analysis of the course of wounds inflicted by animals showed that morphological signs of developing complications of the wound process begin to appear within the next 4-6 hours after the bite and can even lead to the development of a purulent process at such an early date. The combination of microbial contamination of a bite wound with gross anatomical damage increases the risk of developing purulent complications, leading to a long course of the wound process and sepsis.
According to V.V. Oster and V.F. Chikina (1990) abrasions caused by animals suppurated in 6% of cases, superficial wounds - in 9.6%, deep wounds all healed through suppuration.
A high risk of developing infectious complications occurs with bitten hand frames, joints, deep wounds of the face, head, neck and ears. A particularly high risk of suppuration occurs with wounds received in a fight when the teeth are hit with a fist.
Good blood circulation improves and speeds up the cleansing of the bite wound, which reduces the risk of infection.
Bites on the hand usually have a high risk of infection due to the relatively poor blood supply to many structures in the hand. Also, the peculiarities of the anatomical structure of the hand make adequate wound treatment technically difficult. Injuries to the hand and fingers, including bite wounds, often lead to dysfunction of the hand, loss of ability to work, and even disability of the victim.
According to A. Stradi el al. (1988) the risk of developing infectious complications with bites on the hand is 60-65%, with bites on the shin - about 4%, and with bites on the face reaches 35-37%.
Bite wounds on the foot are less common than on the hands or legs. However, the complexity of the biomechanics of the foot, the peculiarities of its lymphophlebodynamics, associated with a high susceptibility to gravitational forces, create difficulties in the surgical treatment of purulent wounds of the foot and further rehabilitation of patients.
In case of damage caused by animals, it is possible to become infected with another dangerous infection - tetanus. Therefore, everyone who has been bitten by animals or humans needs emergency tetanus prophylaxis. More than 4% of cases of tetanus develop after bites, especially after bites to humans.
The pus is green and has a foul odor
If you have a wound or deep scratch on your body, there are two things you need to watch closely: color and smell. If you see green pus oozing from the wound or a foul odor coming from it, this is a sign that you have a purulent infection. You need to urgently run to the doctor. But what if a yellowish film-like substance has formed on a wound or scratch? No need to worry. Doctors say it's actually called granulation tissue, which is part of the healing process. However, it should not be confused with pus.
What is an infected wound and how to treat it?
Every person at least once in his life has had to experience for himself what an infected wound is and how long and painstaking the process of its treatment is. According to the classification of injuries, this type of wound is the most dangerous; if treated incorrectly and late, it can cause enormous harm to health, including amputation of limbs or death.
This form of infection in wounds is caused by an imbalance between the microbes that enter the wound and the body’s protective properties. Infection develops especially often in people suffering from diabetes mellitus and circulatory disorders due to weakened immunity, which cannot fully resist the disease process. Abrasions and broken knees in children are also a cause for concern.
Signs of purulent wounds
There are times when it is not possible to provide first aid or treat the injury site, and then suppuration begins in the wound. Pyogenic bacteria infect the wound, and as a result, general blood poisoning occurs, which can have disastrous consequences for the victim.
A clear sign of an infected wound, that is, the presence of an infection in it, is the accumulation of discharged manure. There are some features of purulent wounds that help to recognize them among other types of damage.
The main signs of infection in a wound are:
- Pain in the wound area, which is throbbing and aching.
- There is noticeable swelling around the wound.
- Redness around the wound at a distance of 1-2 cm.
- An increase in body temperature above 37°C indicates that the infection has begun to spread throughout the body.
- it is necessary to stop the bleeding (apply a bandage or tourniquet);
- treat the skin around the wound with a clean swab with an antiseptic (alcohol, iodine, hydrogen peroxide);
- treat the wound itself with chlorhexidine, a solution of potassium permanganate or hydrogen peroxide;
- apply a sterile bandage.
These symptoms can be supplemented by general disorders throughout the body: dizziness, nausea and weakness.
The period of the first 6-8 hours is especially dangerous for humans and favorable for infection, when the pathogenic properties of microbial contamination are more strongly expressed. The presence of dead tissue is favorable for the development of infection.
In case of severe purulent infection, the body responds with a general reaction depending on the nature and scale of the local process. As soon as symptoms appear in the form of edema and phlegmon, this reaction intensifies. Its striking representative is fever, which manifests itself in the deterioration of the patient’s well-being, increased pain in the wound, changes in the blood (an increase in leukocytes, the appearance of protein and hyaline casts).
Return to zmist Composition when infected with a purulent infection
A serious complication when contracting a purulent infection is sepsis - a general infection of the body with microbes that have entered the blood.
This disease occurs against the background of a violation of protective immunological reactions or during a long, advanced course of a purulent wound process. With sepsis, there is a different incubation period, which can last from two days to several months.
This condition is divided into acute, subacute and chronic sepsis. In severe cases, acute sepsis can result in the death of the patient in a period of 2 days to 2 weeks, subacute - from 16 days to 2 months, chronic - from 2 to 4 months.
Acute sepsis is characterized by high temperature, which is accompanied by fever. The patient's condition is classified as serious. The skin takes on an earthy tint. In patients, the pulse is weakly palpable, tachycardia begins, blood pressure decreases, anemia increases, and signs of leukocytosis appear. The condition of the wound is dry, with pale granulations, it bleeds easily, and a white coating appears. At the slightest suspicion of sepsis, doctors perform immediate surgical intervention. This is the most effective way to save a patient's life.
Return to zmistIkuvaniya infected wounds
If purulent discharge begins to appear in the wound, this indicates that it has become infected. For rapid wound healing, the infection must be suppressed by providing the victim with the necessary assistance. First, you need to ensure the drainage of pus. If it has accumulated under a crust that has formed on the wound, it is soaked in hydrogen peroxide and removed using a bandage soaked in peroxide or another antiseptic, applied for half an hour. If pus is secreted under the skin, it is squeezed out of the hole, which is made along the edge where the flap of skin has dried.
Mandatory procedures include daily wound treatment with hydrogen peroxide. If necessary, the pus should be squeezed out. Levomekol ointment is a good remedy that promotes the healing of an already cleaned wound. It is recommended to apply a bandage with this ointment to the wound daily.
In case of acute suppuration (phlegmon, abscess), surgical intervention is resorted to. The wound is opened with a scalpel, non-viable tissue is excised, and wound discharge is collected for laboratory testing of the microflora and its sensitivity to antibiotics. The wound is washed and dried several times, then tampons soaked in saline solution are applied to the place where the wound is rotting. For some patients with severe pain, saline solution is replaced with novocaine solution. Sutures are placed, which, if healing results are good, are removed on the ninth day.
Doctors very successfully use wipes with immobilized trypsin to heal purulent wounds, thanks to which local manifestations of inflammation disappear after several times of using the solution. On the first day, pain disappears, wound contents peel off, and blood counts improve. The time required for wound cleansing and further treatment after using these medications is reduced by half. High efficiency, effectiveness and ease of use are the main characteristics of immobilized trypsin preparations.
For certain indications, patients are prescribed analgesics, antihistamines and detoxification agents. It is recommended to take immune stimulants throughout therapy. If there is a threat of infection spreading, according to bacteriological tests, doctors prescribe antibiotics. Monitoring the progress of the recovery process, treatment and adaptation in the postoperative period is carried out by doctors during dressing procedures.
Much attention is paid to the severity of inflammatory processes on all sides of the wound, to the study of wound material and the patient’s blood, as well as to studies of the microbial spectrum. Doctors pay special attention to patients with diabetes and people with problems in the circulatory system. Their treatment follows a different scheme and has a number of features due to the complexity of wound healing.
Return to the list First aid instructions
In the field, treatment of infected wounds consists of several stages. If the victims are on a hike, on vacation in the forest or mountains, where there are no medical facilities, then the entire treatment process lies with the team. To do this, it is worth remembering a few recommendations aimed at providing first aid when receiving a serious wound:
If the wound is serious, it will light up within a few days. To treat it, you need to urgently consult a doctor in a nearby locality.
When leaving places of civilization for a long time, you need to have a supply of medical supplies with you for first aid: antiseptics, Vishnevsky ointment, Streptocide, Syntomethacin. And, of course, it is imperative to remember that active, timely treatment with complex and differentiated therapy, the inclusion of modern methods of rehabilitation measures will help speed up the healing process of wounds complicated by infection. A negligent attitude to health problems can lead to irreparable disaster.
You're not feeling well
Although it seems like signs of a skin infection will only appear on your skin, this is not always the case. As the infection spreads, your body mounts a counterattack. And it can lead to systemic symptoms such as fever, nausea, mental confusion or just mild malaise. Although everything is purely individual, if you feel unwell and your wound does not heal for a long time, consult a doctor. Let him examine the wound and study your symptoms. An abrasion or scratch may become a more serious problem.
When your infection becomes something more serious
Skin infections can become serious and can happen literally overnight. Staphylococcus is a good example. Infections are caused by staph bacteria, microbes that are commonly found on the skin of healthy people. This is usually not as problematic when bacteria invade your body. But a staph infection can be fatal to humans. There are many types of infections caused by staph bacteria. They are characterized by redness, swelling, ulcers and usually affect areas of the skin on the legs. Impetigo is a dangerous skin disease caused by staphylococcus bacteria. This is a contagious and painful rash that usually results in large blisters, oozing fluid, and a golden crust. Be sure to see your doctor if you have any of these symptoms or suspect that the infection has gotten worse. The doctor will prescribe antibiotics and treat the lesion to improve your condition.
Wounds begin to fester when pathogenic organisms enter them from the external environment. They end up there immediately after an injury, if it is caused by a dirty object (primary infection) or get inside as a result of violation of the rules of dressing and treatment (secondary infection).
The infectious process leads to inflammation and pain, interferes with normal tissue healing and can spread further, leading to intoxication of the body and sepsis. It is important to recognize the signs of infection in time and eliminate it as soon as possible. In this article we will talk about the treatment of purulent wounds at different stages of the inflammatory process.
Shulepin Ivan Vladimirovich, traumatologist-orthopedist, highest qualification category
Total work experience over 25 years. In 1994 he graduated from the Moscow Institute of Medical and Social Rehabilitation, in 1997 he completed a residency in the specialty “Traumatology and Orthopedics” at the Central Research Institute of Traumatology and Orthopedics named after. N.N. Prifova.
Pathogenic microorganisms easily enter an open wound, but our body has its own defense mechanisms against infection, so the inflammatory process does not always develop. Usually the damage heals successfully, but there are factors that push it to fester. They are conventionally divided into three groups: those related to the wound, the body as a whole, and external conditions.
Wound characteristics that complicate healing:
- Initial contamination, foreign elements in the wound cavity;
- Deep, convoluted wound channel, cavities under the skin with a narrow exit to the outside (there is a risk of infection with anaerobic bacteria, exudate does not drain well and accumulates inside);
- Formed hematoma (blood is an excellent medium for the proliferation of pathogenic microflora).
Body characteristics:
- Immunodeficiency conditions, congenital and acquired;
- Chronic vascular diseases, diabetes mellitus;
- Exhaustion of the body due to illness, poor nutrition;
- Children's and old age
Unfavorable external conditions:
- Improper wound treatment or lack thereof;
- Being in unsanitary conditions (dirt, high humidity).
So, you should be especially attentive to complex wounds, contaminated or irregularly shaped, and take into account the general condition of the body in order to prevent negative reactions.
Infected wounds are always an unpleasant surprise. In itself, a violation of the integrity of the skin does not pose a danger to humans, but if bacterial flora is added to this, an inflammatory process begins, which is accompanied by an increase in local temperature, redness, pain and dysfunction of the limb and/or organ on which the wound is located.
Definitions
A wound is a mechanical violation of the integrity of the skin or mucous membranes. Possible damage to the underlying tissues and an increase in the traumatic condition. This is one of the types of injury that always poses a threat to human life and health. It is the most important aspect of study in surgery. A wound is a traumatic situation that leads to the appearance of a wound.
Clinic
The symptoms that accompany infected wounds depend on their number and severity of the condition. There are several local signs inherent in any injury of this kind.
- Pain. At the moment when the integrity of the skin is disrupted, nerve endings are damaged, and a significant amount of cytokines and prostaglandins are released, which stimulate unpleasant sensations. The sensitivity of tissues in different parts of the body is the same. It is most pronounced in the nerve trunks, periosteum, in the pulp of the tooth, in the peritoneum and pleura. Parenchymal organs, like the brain, do not have pain receptors.
- The gaping of the wound depends on its width and depth, as well as on the number of torn fibers. It is most observed when muscles and a significant fat layer are damaged.
- Bleeding. This sign is closely related to the site of injury. If large vessels are damaged, especially arteries, then blood loss will be significant, but rupture of capillaries will not cause significant harm to health.
- aseptic (after primary surgical treatment);
- contaminated (microbial bodies, but no signs of inflammation yet);
- infected (redness, swelling, local fever, pain and changes in function are present).
- primary intention (the wound is clean, shallow, caused by a sharp object);
- secondary intention (large number of granulations, infected wounds);
- healing under the scab (coagulative necrosis from a chemical burn).
- complete cleansing of the wound;
- antiseptic treatment;
- installation of drainage for better outflow of infected fluid;
- stimulation of the local immune system.
If a superficial wound is inflicted, the overall reaction of the body will be insignificant. But with multiple deep incised wounds, the symptoms will be determined by the location of the injuries, the degree of blood loss and the addition of a secondary infection. This is dangerous due to the development of hemorrhagic or hypovolemic shock, cerebral hypoxia, sepsis and other complications.
Classification of wounds
For doctors, there is a unified directory of diseases, in which an infected wound is listed. ICD 10 assigned it the code T80-T88. This section is responsible for human injuries and their complications. But there is another classification. For example, based on the nature of the weapon, a gunshot wound and a knife wound are distinguished. Based on the cutting edge of the traumatic agent, the following types can be distinguished: punctured, cut, chopped, torn, bitten, bruised, crushed, and so on. Based on the shape of the resulting defect, linear, patchy, and perforated damage is noted. Based on the depth of penetration of the traumatic agent, superficial, penetrating, through and tangential wounds are distinguished. There is a classification that indicates the degrees into which an infected wound is divided (ICD 10 does not distinguish this):
The healing of a wound depends on why it was inflicted. There are three options for the development of events:
Wound process
The wound process is the sequential changes that occur in the wound during the process of its receipt and healing, as well as the body’s reactions caused by this process. They are aimed at delimiting the source of infection from the vascular network and removing all pathological agents from it. The universal way that nature has come up with to protect a person from the consequences of injuries is an inflammatory reaction. The first phase of the wound healing process is based on the physical response of the tissue to injury. Immediately after injury, the death of some tissues, their destruction and cavitation, as well as the formation of hematomas are observed. In the first seconds, vascular spasm occurs, which is replaced by a sharp dilation of blood vessels and bleeding. After a short period of time, blood flow slows down and a blood clot forms. In parallel with this, inflammatory mediators accumulate in the wound, which attract leukocytes, phagocytes and mast cells. Bacteria accidentally introduced onto the wound surface are eliminated and absorbed by local cellular immunity. After some time, an inflammatory mass of dead cells and swelling appear around the wound. The vascular network contracts, and secondary necrosis forms. It is at this moment that pain appears and the function of the affected area is disrupted. The second phase of the wound process occurs after three days, but there is no clear boundary. The inflammatory process continues, and soft tissue injuries result in an infected wound. The ICD code changes by several points. Mechanical cleansing of the wound stimulates the growth of granulation tissue, and the removal of dead bacteria by phagocytes reduces inflammation. The regeneration process begins, new blood vessels are formed, dense collagen tissue grows, and a fresh, soft scar appears at the site of the wound. After ten to fourteen days, the third phase begins - scarring and epithelization. Collagen filaments become more and more dense, the vessels no longer sprout. At the same time, the epidermis layer is formed. The new scar has a soft pink color, but over time the capillaries disappear and it fades, becoming almost invisible. According to this scheme, everything heals, not just infected wounds. Of course, there are always individual variations in these three phases.
The body's response to an infected wound
The general reaction can be divided into catabolic and anabolic phases. During the first (up to the 4th day), all vital processes intensify: the temperature rises, metabolism accelerates, a person loses weight, protein synthesis is inhibited and the permeability of cell membranes decreases. The body is adjusted to regeneration. The second phase begins on the fourth day after the injury, and everything gradually falls into place. Body weight is restored to the previous level, metabolism is normalized, and with it the temperature drops. The activity of adrenal hormones increases slightly.
Wound healing
Each tissue has a certain tendency to regenerate. Not all cells are equally good at producing their own kind, especially if it is an infected wound (the ICD does not make any recommendations on this matter). The speed and quality of healing depends on the conditions in the affected area. If it is dry, clean and free of foreign bodies or bacteria, the process will proceed faster. And, accordingly, vice versa. The general condition of the body also affects the rate of regeneration. In young and healthy people, healing is easier, but the presence of chronic diseases, large blood loss or vitamin deficiency can worsen the course of the disease and delay the recovery process for several weeks, or even months.
Surgical treatment of wounds
The purpose of primary surgical treatment is mechanical cleansing of the wound from necrotic tissue, foreign bodies and bacteria. Treatment of infected wounds begins with the skin around the damaged area being wiped with a cotton or gauze swab soaked in alcohol/saline, and then treated with a one percent iodine solution. The surgical field is covered with sterile napkins, and after anesthesia, the edges of the wound are moved apart and moved apart. This is necessary to make it easier to remove foreign bodies and dirt. For example, if a patient has an infected foot wound, then most likely there are particles of earth in it. Necrotic tissue is excised. If necessary, the wound can be enlarged for better access to all blind spots and possible pockets. If large vessels are damaged, they are ligated and the nerves are sutured. After the surgeon has finished removing all excess, the wound is sutured tightly and an aseptic bandage is applied. Some exceptions are mentioned in the ICD. An infected foot wound, for example, must remain open because the soil with which it was contaminated harbors anaerobic bacteria that cause decay. The gaping damage ensures constant access of oxygen to the tissues, which means it does not allow microorganisms to develop.
Therapy of purulent wounds
Clinical signs by which it can be determined that a person, for example, has an infected leg wound, appear on the second or third day from the moment of injury. This is facilitated by the presence of signs of inflammation and pathogenic or opportunistic flora. When treating such injuries, one should focus on the type of bacteria and select an antibiotic that matches the sensitivity. The general approach is:
General treatment
Antibiotics remain the cornerstone of treatment for infected wounds. The drug, route of administration, dose and frequency of administration directly depend on the microorganism that caused the suppuration. If the flora is anaerobic, then it is best affected by metronidazole and clandomycin in combination with sulfonamides. Impaired immune function, both local and general, affects the healing process, so it is necessary to maintain it at the right level. Mobilization of the body's protective factors helps to avoid complications such as sepsis, fever and others.
Signs of inflammation
They are also divided into two groups: local and systemic.
Note that the infection does not remain local for long - only 6-9 hours.
Pathogenic microorganisms and toxic products of their vital activity spread with the lymph flow, causing a reaction throughout the body.
The first signs of inflammation:
- The skin at the site of injury becomes hot;
- Redness occurs around the wound;
- Edema and swelling form along the edge;
- An aching, throbbing pain is felt, which intensifies when you press the edge of the wound with your finger.
As the infection spreads through the lymph flow, general symptoms develop:
- increased body temperature;
- weakness and lethargy;
- increased heart rate;
- leukocytosis;
- enlargement and tenderness of the lymph nodes closest to the wound.
When infected with pathogenic microorganisms, pus appears at the site of the lesion. At first it is liquid and flows out of the wound, then it thickens. Pus has an unpleasant odor, the shade depends on the nature of the microflora. It is usually yellowish or greenish.
When inflammation becomes chronic, a purulent focus with granulation tissue along the edge is formed - an abscess (abscess). If the wound breaks, the help of a surgeon is required to open the abscess.
Complications of wounds. Basic principles of treatment. Infectious complications of wounds
Complications of wounds are divided into early and late.
To the early
complications include primary bleeding, injuries to vital organs, traumatic or hemorrhagic shock.
By the later
complications include early and late secondary bleeding,
seromas - accumulations of wound exudate in wound cavities, which are dangerous due to the possibility of suppuration.
When a seroma forms, it is necessary to ensure the evacuation and drainage of fluid from the wound.
Wound hematomas
are formed in wounds closed with a suture due to incomplete stopping of bleeding during surgery or as a result of early secondary bleeding. The causes of such bleeding may be increases in blood pressure or disturbances in the patient’s hemostatic system. Wound hematomas are also potential foci of infection; in addition, by squeezing tissue, they lead to ischemia. Hematomas are removed by puncture or open exploration of the wound.
Necrosis of surrounding tissues
— develop when microcirculation in the corresponding area is disrupted due to surgical tissue trauma, improper suturing, etc. Wet skin necrosis must be removed due to the danger of their purulent melting. Superficial dry necroses of the skin are not removed, as they play a protective role.
Wound infection
- its development is promoted by necrosis, foreign bodies in the wound, accumulation of fluid or blood, disruption of local blood supply and general factors influencing the course of the wound process, as well as the high virulence of wound microflora. There are pyogenic infections, which are caused by staphylococcus, Pseudomonas aeruginosa, Escherichia coli and other aerobes. Anaerobic infection, depending on the type of pathogen, is divided into non-clostridial and clostridial anaerobic infection (gas gangrene and tetanus). Erysipelas is a type of inflammation caused by streptococcus, etc. The rabies virus can enter the body through bite wounds. When a wound infection generalizes, sepsis may develop.
Dehiscence of wound edges occurs
in the presence of local or general factors that impede healing, and when the sutures are removed too early. During laparotomy, the divergence of the wound can be complete (eventration - exit of internal organs to the outside), incomplete (the integrity of the peritoneum is preserved) and hidden (the skin suture is preserved). Dehiscence of the wound edges is eliminated surgically.
Complications of wound scarring
can be in the form of the formation of hypertrophied scars, which appear with a tendency to excessive formation of scar tissue and more often when the wound is located perpendicular to the Langer line, and keloids, which, unlike hypertrophied scars, have a special structure and develop beyond the boundaries of the wound. Such complications lead not only to cosmetic, but also to functional defects. Surgical correction of keloids often leads to a deterioration of the local status.
In the practical work of a military pathologist, there were often various kinds of disturbances during the speech process, such as: a significant prolongation of the healing period of wounds, which required new medical interventions and in some cases posed a direct threat to the life of the wounded.
The concept of “complication of a wound process” is inextricably linked with the reactivity of the body with its ability to localize the process within the wound zone, i.e. with the potential ability of its tissues to undergo both inflammatory and regenerative processes. The volume and nature of the injury, as well as the nature of its surgical treatment and subsequent care, are of great importance. Wounds with a complex profile and a large area of traumatic necrosis are much more often accompanied by complications than with little trauma to surrounding tissues. Various complications during the healing of soft tissue wounds can be divided into two main groups. In the first of these, changes in the wound are largely subordinate in nature, reflecting changes in the general condition of the wounded. In the second group of complications, the wound itself is the main starting point for immunobiological changes. Pathological processes primarily arise in it and cause a reaction of the whole organism.
The first group includes atypical wound healing in debilitated individuals in the presence of various kinds of diseases, in the presence of another wound playing a leading role in the wound process, with vitamin deficiencies, etc. It is also necessary to note the possibility of an inverse relationship. The atypical course of wound healing under the above conditions can, in a certain period, acquire a leading role and determine the outcome of the wound process. An example of this is the development of septicemia in the exhausted, when they have flaccid granulating wounds. However, a large, long-festering wound determines a change in the general reactivity and metabolism of the wounded person and ultimately acquires the main features of dystrophic wounds. Consequently, the relationship between the general state of the body and the local process is not constant and established once and for all. The idea of reactivity is inextricably linked with the nutritional status of the wounded person, various combinations of vitamin deficiencies, his age, etc. This issue is currently widely covered in the domestic literature. Here it is advisable to dwell only on local pathomorphological changes in the wound itself.
In a war situation, it was often possible to observe the perverted course of reparative processes in wounds of exhausted people. Exhaustion itself had different etiologies. In some cases it was the result of insufficient or malnutrition, in others it was the result of debilitating and long-term diseases; finally, thirdly, as a consequence of protracted purulent wound processes leading to severe metabolic disorder and dystrophy, figuratively called “wound consumption” by N. I. Pirogov.
At present, we can definitely state that pathological changes in the tissues and organs of exhausted people, regardless of the cause that causes them, are largely identical. A number of authors provide evidence of this position (I.V. Davydovsky, A.V. Rusakov, A.P. Avtsyn, P.E. Snesarov, etc.). Accordingly, the similarity in the morphological manifestation of tissue reactions is determined. What is common to the wound process in the exhausted is the extremely sluggish nature of the reparative processes, a tendency to necrosis in the wound, a large number of bacteria in dying tissues and the frequent development of septic complications. According to N.F. Melnikov-Razvedenkov, with dystrophies, swelling of the connective tissue base occurs, followed by degeneration of its elements, hydrolytic vacuolization and, finally, complete histolysis of tissue structures. This explains not only the atypia of the tissue response to injury, but also the possibility of secondary opening of already healed wounds. A gunshot wound with severe dystrophy seems peculiar in appearance. Delay and cessation of growth and maturation of granulations are replaced by necrobiotic and necrotic changes in them. Granulations become scarce, their layer becomes thinner. Graininess disappears. The wound surface turns pale and acquires either a dryish gray appearance or a moist appearance. In the latter case, the wound becomes covered with a greenish sticky mass. Necrotic changes are already determined macroscopically in the form of loosening of granulation areas and their transformation into a dirty, decaying mass. Ulcerations of granulations in some cases are so extensive and deep that the fascia underneath is often exposed.
Histological examination of the wound shows that the basis for the disappearance of the graininess of granulations is not their maturation, but the desolation of blood vessels and the death of cellular elements. In this case, the upper layer appears in the form of a structureless layer formed by fibrin and necrotic tissue. Fibrin and necrotic tissues are densely permeated with microbial bodies, which in some places form significant accumulations.
The microflora of such wounds is usually polymorphic; here there are both rods and a wide variety of cocci, differently stained using the Gram method. At the same time, the relatively small number of microbial bodies with an intracellular location attracts attention. The described layer of necrosis and the following layer of necrobiotic changes in granulation are more or less densely permeated with leukocytes, which are also in a state of various stages of decay. In granulations, the vascular network is poorly expressed, the lumens of the capillaries contain bacterial thrombi, and mixed and leukocyte thrombi are found in larger vessels bordering the wound cavity. Similar changes apply to the lymphatic vessels. Capillaries of granulation tissue are widely involved in the necrobiotic process. The endothelium becomes swollen and in some places undergoes decay. A picture of capillary necrosis appears.
The described changes in wounds with dystrophies open up wide opportunities for breaking through wound barriers and cause septic complications. The natural evolution of tissue structures is sharply suppressed and distorted. On the one hand, the death of young elements of connective tissue occurs, on the other hand, the process of converting them into profibroblasts is inhibited. The number of profibroblasts is small and they often show clear signs of hydrotic degeneration, vacuolization and nuclear disintegration. Collagen fibers are difficult to detect. Dystrophic changes in granulations include destructive changes in argyrophilic fibers, expressed in swelling and disintegration into segments and clumps (M.K. Dal), delayed differentiation of cellular elements and the development of polyblasts not in the direction of fibroblasts, but in the direction of irritation cells with a significant increase in the number plasma cells.
In the figurative expression of I.V. Davydovsky, a “dull cytological landscape” arises. The cellular elements are mostly small, round, with a thin, discontinuous reticular network between them. There are few vessels and they are poorly distinguishable. Sometimes such tissue is more reminiscent of lymphadenoid tissue (M.K. Dahl) than granulation tissue. Epithelization of the wound is delayed. The skin around the wound takes on a peculiar appearance, becoming thin, dry, and senile. The marginal zone of epithelialization acquires a bluish tint.
In some cases, manifestations of vitamin deficiency become of particular importance in the morphology of a gunshot wound of soft tissues. The most demonstrative are scurvy changes in wounds. In these cases, a completely unique type of granulation cover appears. Against the general pale background of these granulations, purplish red or cyanotic lesions of various sizes and shapes appear in the form of flat smears or rounded swelling formations. Histological examination in such areas reveals phenomena of apoplexy with an unclear structure of tissue elements and its vessels. Such granulations resemble a sponge soaked in blood.
Along with widespread hemorrhages into the granulation tissue, scurvy changes in the wound are characterized by the constant presence of necrotic and destructive processes. The latter are initially confined to places of hemorrhage, then can spread significantly. Of great importance in the spread of both hemorrhages and necrosis is, on the one hand, the instability of blood circulation in granulations with an imperfect system of their vessels, and on the other, the fragility of intercellular connections. The dead masses are riddled with a huge number of microbes. The reproduction of the latter occurs completely unhindered, just as they germinate in a nutrient medium in a thermostat. Such favorable conditions for the development of flora are partly explained by the lack of vitamin C, which makes the blood more bactericidal and sharply reduces tissue resistance to infection.
The whole process is uneven - in the same wound one can observe the most initial and advanced changes characteristic of scurvy. Fresh hemorrhages are bordered by foci of granulation tissue with cellular necrosis, with a fibrin network between cells, as well as with leached and homogenized red blood cells. The previously bulging, juicy and red area sinks and becomes dry, gray and dull when it is saturated with fibrin. In practice, wounds with pronounced scurvy do not heal.
Studies by M.F. Glazunov and other authors have shown that with such wound complications, it is not so much the proliferation of cellular elements that is disrupted, but their subsequent differentiation. The healing mechanism suffers due to pronounced fibroplasia, a disruption in the formation of collagen fibers. According to the experimental work of V. G. Eliseev, with vitamin deficiency, the emigration of leukocytes into the wound is significantly delayed and their rapid decay occurs. Along with a sharp drop in fibroblastic activity, the resorption of dead materials slows down. In accordance with the general drop in tissue reactivity, the absorption capacity of reticuloendotheliosis fades.
Thus, the regeneration processes in the wound not only slow down, but also become abortive in nature. The formation of persistent tissue structures does not occur, and almost any new manifestation of granulation growth is accompanied by circulatory disorders, apoplexy and necrosis.
Of the local morphological changes in the wound caused by the general reactivity of the tissues, changes in the allergic order should be noted. At the beginning of the Great Patriotic War, A. I. Abrikosov recalled this and the corresponding data was noted by a number of authors based on wartime material.
The morphological manifestation of a hyperergic reaction in a wound is primarily changes in its blood vessels. The walls of the vessels swell and become saturated with a basophilic protein substance and become homogenized. In such cases, they usually talk about fibrinoid degeneration of the vascular wall. The change primarily affects the arteries, in which swelling of the walls leads to a significant narrowing of the vascular lumens. In the most pronounced cases, similar changes occur in the connective tissue fibers. They swell, homogenize and exhibit the same basophilicity as homogenized vascular walls (S.S. Weil). Often in granulations of the described type one can see changes in one or another part of the capillaries with the impregnation of their walls with protein liquid and swelling of endothelial and perivascular cells. These changes in the vessels are replaced by early onset sclerosis.
A.I. Abrikosov points out that allergic changes in the wound often occur in later periods of its existence and during protracted septic processes. S.S. Weil, noting the frequency of such changes, especially emphasizes their importance in the process of wound healing.
The inconstancy of the morphological manifestations of the hyperergic reaction does not at all exclude their practical significance. A wound can suffer not one hyperergic attack, but several, successively following each other (A. I. Abrikosov). In the intervals between attacks, the morphological signs of a hyperergic reaction fade away. Thus, the absence of morphological signs of a hyperergic reaction does not indicate the rarity of the latter. Everything will depend on the phase of the reactive state in which the biopsy material was taken or the death of the wounded occurred and the subsequent study of the cadaveric material was carried out.
At the same time, the transfer of hyperergic attacks does not remain without leaving a mark on the wound. Some forms of atypical fibroplasia of granulations and their early sclerosis can be associated with a similar phenomenon, which will be discussed below.
It should be noted that the physiological characteristics of granulation tissue with great instability and fragility of blood circulation in it contribute to the rapid response of this tissue to all kinds of immunobiological changes occurring in the body of the wounded. When studying biopsy material, a certain synchronicity of pathological phenomena is clearly revealed at the site of development of the main wound process, the tank and in accompanying smaller wounds. The main form of “response” reaction is the manifestation of discirculatory and dystrophic processes. Thus, almost any significant complication at the site of the main wound is accompanied by attenuation of proliferative processes in the accompanying wound, fading of granulations and delayed epithelization. A similar picture arises when any other disease of the wounded person (pneumonia, acute contagious diseases, etc.) joins the wound process. Sometimes the “response” reaction in the accompanying wound is qualitatively adequate to the process that developed in the main wound. So, for example, with acutely developed wound phlegmon, the same picture is reproduced in miniature in accompanying wounds. Deep leukocyte infiltration of granulation tissue occurs. Even more constant is the dependence of hyperergic phenomena in the accompanying wound on the same changes at the site of development of the main wound process. All this once again convinces us that wound healing cannot be considered as a purely local process.
Complications of wounds are divided into early and late.
To the early
complications include primary bleeding, injuries to vital organs, traumatic or hemorrhagic shock.
By the later
complications include early and late secondary bleeding,
seromas - accumulations of wound exudate in wound cavities, which are dangerous due to the possibility of suppuration.
When a seroma forms, it is extremely important to ensure the evacuation and drainage of fluid from the wound.
Wound hematomas
are formed in wounds closed with a suture due to incomplete stopping of bleeding during surgery or as a result of early secondary bleeding. The causes of such bleeding are increases in blood pressure or disturbances in the patient’s hemostasis system. Wound hematomas are also potential foci of infection; in addition, by squeezing tissue, they lead to ischemia. Hematomas are removed by puncture or open exploration of the wound.
Necrosis of surrounding tissues
— develop when microcirculation in the corresponding area is disrupted due to surgical tissue trauma, improper suturing, etc. Posted on ref.RF It is extremely important to remove wet necrosis of the skin due to the danger of their purulent melting. Superficial dry necroses of the skin are not removed, as they play a protective role.
Wound infection
- its development is promoted by necrosis, foreign bodies in the wound, accumulation of fluid or blood, disruption of local blood supply and general factors influencing the course of the wound process, as well as the high virulence of wound microflora. There are pyogenic infections, which are caused by staphylococcus, Pseudomonas aeruginosa, Escherichia coli, etc. Posted on ref.rf aerobes. Anaerobic infection, based on the type of pathogen, is divided into non-clostridial and clostridial anaerobic infection (gas gangrene and tetanus). Erysipelas is a type of inflammation caused by streptococcus, etc. Posted on ref.rf The rabies virus can enter the body through bite wounds. When a wound infection generalizes, sepsis may develop.
Dehiscence of wound edges occurs
in the presence of local or general factors that impede healing, and in case of too early removal of sutures. During laparotomy, the divergence of the wound should be complete (eventration - exit of internal organs to the outside), incomplete (the integrity of the peritoneum is preserved) and hidden (the skin suture is preserved). Dehiscence of the wound edges is eliminated surgically.
Complications of wound scarring
occur in the form of the formation of hypertrophied scars, which appear with a tendency to excessive formation of scar tissue and more often when the wound is located perpendicular to the Langer line, and keloids, which, unlike hypertrophied scars, have a special structure and develop beyond the boundaries of the wound. Such complications lead not only to cosmetic, but also to functional defects. Surgical correction of keloids often leads to a deterioration of the local status.
Complications of wounds. - concept and types. Classification and features of the category “Complications of wounds.” 2020, 2020.
A wound is a gaping violation of the integrity of the skin or mucous membranes. A wound is a violation of the integrity of the skin, mucous membranes (superficial wounds), underlying tissues and internal organs (deep wounds). Wounds that have been subjected to additional exposure to physical, biological or chemical factors (frostbite, burns, hard electromagnetic radiation, microbial contamination, aggressive chemicals, ionizing radiation, etc.) are called combined. Based on the nature of tissue damage, they are distinguished: Incised wounds resulting from exposure to sharp objects (for example, a razor, a knife). The edges of the wounds are even and smooth. The wound is not deep, it gapes. The bottom of the wound is slightly destroyed, unless it is large vessels and nerves, for example, in the neck. Incised wounds are the most favorable for healing. Chopped wounds caused by a sharp but heavy object (axe, saber) resemble cut wounds in their clinical picture. A distinctive feature is more significant destruction of the wound bottom. Usually the adjacent tendons, muscles and even bone are damaged. Puncture wounds resulting from injury by sharp and thin long objects (knife, sharpener, awl, etc.). These are often extremely dangerous wounds, since a small, sometimes pinpoint wound does not gape, does not bleed, and quickly becomes covered with a crust. At the same time, a wounding object could damage the lung, intestines, liver, and after some time anemia, pneumothorax or peritonitis are possible.
· Bruised wounds resulting from exposure to a blunt object (stick, bottle). The edges of the wound are crushed, as are the tissues in the wound itself. The latter are soaked in blood, dark in color, do not bleed or bleed slightly. Visible vessels are thrombosed. Lacerations that occur when a relatively sharp object slides across the surface of the skin with additional pressure on it. The wound is irregular in shape, with scalp-type flaps, and bleeding. The destruction of the underlying tissue depends on the force exerted on the wounding projectile. Typically, lacerated wounds, as well as bruised wounds, have a protracted healing process due to necrosis of destroyed tissue and suppuration in the wound. Poisoned wounds that occur when toxic substances enter them (snake venom, toxic substances). Gunshot wounds, which differ from all others in the characteristics of the wounding projectile, the wound channel and the course of the wound process.
Based on the reasons for damage, wounds are divided into operating wounds; random.
Wounds are classified according to microbial contamination: antiseptic; microbially contaminated.
It is important to take into account the location of wounds (abdominal cavity, head, limbs, etc.) and the type of damaged internal organs (liver, intestines, lung, spleen, etc.) and tissues (bones, muscles, nerves, joints, blood vessels). During the wound process When healing purulent wounds, it is advisable to distinguish the following stages: 1) inflammation, 2) formation and maturation of granulation tissue, 3) epithelization.
The identification of stages, despite their specific sequence, is conditional, since it is impossible to draw a strict line between the end of one stage and the beginning of another. Granulation tissue usually appears within 48 hours. After the inflammatory reaction subsides, the process of transformation, proliferation of fibroblasts, formation of new tissue begins - the process of reparative regeneration. Throughout the inflammatory reaction, starting from the moment of tissue damage, proliferative or productive phenomena (reproduction of cellular elements) are observed. These phenomena are especially pronounced in the later stages of inflammation. As granulation tissue grows, connective tissue forms and matures, inflammatory phenomena subside, and epithelization occurs from the edges of the wound to its bottom. Since wounds make up the majority of injuries to the body, their treatment is the basis of first aid for injuries.
First medical aid is a set of emergency simple measures aimed at saving a person’s life, as well as preventing possible complications in the event of an accident, carried out directly at the scene of the incident by the victim himself or another person who was nearby.
Protecting a wound from infection is best achieved by applying a bandage while observing the following rules: · do not touch the wound with your hands, since there are especially many microbes on the skin of the hands; · the dressing material used to close the wound must be sterile.
We also recommend
- Inclined lifts for disabled people
- Types of stair lifts for the disabled
- Okof lifting platform for disabled people
- Why do you need quartzing of the throat and nose?
- Okof ramps for disabled people in budgetary institutions
- Lingerie after mammoplasty Compression tape after mammoplasty
Wound treatment methods at different stages
Treatment of infected wounds is divided into local and systemic.
Please note that systemic drug treatment is prescribed only by a doctor.
This includes detoxification therapy, taking antibiotics, immunomodulating drugs, vitamins, etc.
Local treatment is organized according to the phases of the wound process. At each stage, different techniques and medications are used.
Treatment in the inflammatory phase
In the inflammation phase, the wound “gets wet” - liquid exudate is released, later pus appears, and part of the tissue dies. When treating such a wound in a hospital, the surgeon washes it with an antiseptic, removes pus and necrotic tissue, installs drainage to drain exudate, and applies a sterile bandage soaked in the same antiseptic solution. The dressing is changed every 5-6 hours, the wound is re-treated daily until granulation begins.
Surgical wounds that have festered during treatment are washed, the sutures are removed, and the edges are pulled apart.
At home, small inflamed wounds on the arm or leg are dealt with in the same way: washed, cleaned of pus, applied with a napkin soaked in an antiseptic, and wrapped with a sterile bandage.
Ointments are not used at this stage - they prevent the outflow of fluid.
Typically, water-soluble gel and ointment preparations are added on the 3rd day.
The dried bandage is pre-soaked. After washing, the ointments are applied to a sterile napkin and wrapped with a bandage.
To treat necrotic wounds, proteolytic enzymes are used, which dissolve dead tissue and reduce inflammation (chymopsin, chymotrypsin, trypsin). They are used in the form of powders or solutions. To quickly remove purulent discharge, a sorbent (polyphepan, celosorb) is placed in the wound.
Today, new, progressive methods of cleaning wounds are used in hospitals:
- laser processing;
- vacuum removal of pus;
- ultrasonic cavitation;
- cryotherapy;
- pulsating jet treatment, etc.
Laser treatment of wounds
Treatment in the granulation (proliferation) phase
During this period, the inflammation gradually subsides, the wound is cleared of necrotic tissue and pus, and the amount of discharge decreases. The drainage is removed, and absorbent dressings and rinsing are no longer needed. If required, at this stage the surgeon applies secondary sutures, or the edges of the wound are closed with adhesive tape.
Treatment includes ointments with anti-inflammatory, regeneration-stimulating and antibacterial properties.
Treatment in the epithelization phase
At this stage, the wound heals, new thin epithelial tissue appears, and a scar is formed. The wound is protected from damage, using ointments and creams that soften and stimulate regeneration and prevent the formation of a rough, tightening scar.
Treatment of infected wounds
Therapeutic measures for wound infections should be aimed at clearing the surface of non-viable and necrotic tissue, eliminating swelling, restoring microcirculation, and suppressing the pathogen. For this purpose, surgical and conservative treatment methods are used.
Surgical treatment consists of secondary surgical treatment, drainage, and suturing.
Treatment of an infected wound is carried out on days 4-5, since during this period secondary necrosis completes its formation.
Surgical treatment consists of dissection of the injury and excision of necrotic tissue. During surgical treatment of wounds, it is recommended to use general anesthesia, especially for extensive purulent injuries, since local anesthesia is not enough to remove all non-viable tissue, perform drainage or apply sutures.
Drainage is done to ensure the outflow of serous exudate and pus. Drainage helps clean the wound and also deprives pathogenic flora of a nutrient medium.
Treatment for a wet surface is as follows:
- Change the dressing as soon as it gets wet, after 5-6 hours;
- Treatment of the wound with furatsilin, Furazol spray;
- Application of 10% sodium chloride solution, 4% sodium bicarbonate, 3% boric acid;
- Use of liquid antiseptics: Miramistin, Miramidez, Betadine, Octenisept, Iodinol.
Fudizin gel, streptocidal, zinc ointment, sulfonamide antimicrobial ointments (Mafenide, Streptonitol), Solcoseryl gel are used under the dressing.
Procedure for treating a purulent wound:
- Avoid accumulation of purulent exudate and remove it regularly;
- Use Trypsin, Terrylitin, Himopsin powders, Profezim suspension;
- The powders are mixed with novocaine and sodium chloride, sterile napkins are impregnated with it, which are placed into the wound cavity;
- For deep wounds, powders are used dry;
- To combat pathogenic bacteria, antibiotics are used orally, intramuscularly or intravenously;
- They use ointments that act on bacteria.
Ointments are used under a bandage, water-based liniments are applied, such as Levosin, Levomikol, Sintomycin, Baneocin, Nitacid, Solcoseryl.
Oil-based ointments or Vaseline are rarely used. In a hospital setting, patients undergo detoxification and immunotherapy, and are also treated with liquid nitrogen, ultrasound or HBOT. You will learn further about how you can treat an infected wound at home.
Review of wound treatment products
Today, pharmacies offer many drugs for the treatment of wounds. Let's look at the most frequently used ones.
Wash solutions:
- boric acid 3%;
- chlorhexidine 0.02%;
- dioxidine 1%;
- miramistin;
- furatsilin, etc.
Antibacterial gels and ointments on a water-soluble basis:
- Levosin;
- Solcoseryl gel;
- Levomekol;
- Dioxidine;
- Methyluracil with miramistin.
These drugs accelerate the cleansing of the wound from dead parts and pus, destroy pathogenic microorganisms, and stimulate granulation. They are applied in a thin layer once a day, placed in the wound with a sterile napkin or inserted into the drainage.
Antibiotic ointments:
- Gentamicin;
- Syntomycin.
These are inexpensive bactericidal drugs with a wide spectrum of action for the treatment of non-healing wounds, abscesses, and ulcers.
Ointments with regenerating and anti-inflammatory properties:
- Solcoseryl;
- Actovegin
They improve metabolism and cellular metabolism, accelerate epithelization, reduce inflammation, and create a protective film on the surface.
Complex action drugs:
- Oxycyclosol (aerosol containing oxytetracycline and prednisolone);
- Oxycort and Hyoxysone (aerosol and ointment with oxytetracycline and hydrocortisone)
Scar creams:
- Contractubex;
- Dermatix;
- Zeraderm.
Infectious complications of gunshot wounds (part 1)
Author: Artem Kutsenko, Medsanbat trainer
All gunshot wounds are primarily contaminated with various microbial associations, including anaerobic ones. An unsutured wound heals by secondary intention with the formation of granulations. The development of wound infection is predisposed by the application of primary sutures after non-radical surgical treatment. Non-radical surgical treatment of a gunshot wound is characterized by insufficiently rational dissection of the wound, leaving unopened fascial sheaths, non-viable tissues, foreign bodies, projectile fragments, free bone fragments, as well as poor hemostasis. The development of purulent wound infection can lead to severe deformation of the limbs. Violations of not only the general protective reaction of the body, but also local wound immunity, when the susceptibility of tissues to microflora changes, are also important. Its composition, as well as the number of microbes in the wound, play an important role in the occurrence and course of the infectious process.
The species composition of the wound microflora often changes. About 80% of microbes cultured from a wound are antibiotic resistant. The demarcation barrier formed at the border of living and dead tissues often prevents the spread of microbes deep into living tissues and leads to limited suppuration, followed by gradual healing of the wound by secondary intention.
The presence of microbes in a wound healing by secondary intention always poses the danger of infection spreading beyond the line of demarcation inflammation into viable tissue along the wound canal and creates a threat of progression of the purulent-inflammatory process with the development of both local and general purulent infection. In the system of complex treatment of wound infection, surgical intervention plays a leading role.
Wound infection is an infectious process that develops in living tissues surrounding the wound, under the influence of microbes that penetrated it at the time of injury and after some time is accompanied by damage and death of cellular structures with the formation of new foci of necrosis and a clinically expressed general reaction of the body.
Options (depending on damage level):
- Cellular and tissue (primary foci of damage).
- Organ-systemic (organs and systems at a distance from the primary focus).
- Organismal (generalized forms of infection that affect the body as a whole).
Acute forms:
- Aerobic (purulent) infection
a) suppuration of the wound
b) wound infection
– abscess of the wound channel, cavity, organ;
- periwound phlegmon (in the form of cellulite, myositis, fasciitis, osteitis or combinations thereof).
- purulent swelling.
- Anaerobic infection:
a) monoinfections:
b) polymicrobial (synergistic) infections.
Chronic forms:
- Chronic suppuration:
a) soft tissues (arising due to the long-term existence of purulent cavities containing bone and/or soft tissue sequestration; foreign bodies).
b) bedsores (arising as a result of long-term disruption of tissue trophism).
- Chronic wound infection (open, closed and fistula forms):
a) fasciitis
b) tenosynovitis
c) osteomyelitis
- Chronic polymicrobial infections:
a) progressive synergistic bacterial gangrene;
b) chronic perforating ulcer.
II. Visceral infectious complications - develop at a distance from the primary focus.
- CNS: (meningitis, encephalitis, meningoencephalitis)
- Respiratory organs: (tracheobronchitis, pneumonia)
- Cardiovascular system: (thrombophlebitis, myocarditis, endocarditis).
- Gastrointestinal tract: (pancreatitis, cholecystitis).
- Urinary system: (nephritis, pyelonephritis, cystitis, urethritis)
- Systemic connective tissue lesions: (pleurisy, synovitis, polyarthritis, ascites, pericarditis).
III. Generalized infectious complications are the loss of the body’s ability to localize and suppress pathogens of wound infection outside the infectious focus.
- Sepsis.
- Severe sepsis (including diffuse peritonitis).
- Septic shock.
Development of an infectious complication
- The presence of five classic signs of inflammation in the wound area: pain, hyperemia, swelling, fever, dysfunction.
- Manifestation of systemic inflammatory process syndrome (SIPS).
- A combination of the first and second signs. The first variant of clinical manifestations corresponds to local infectious complications. In the second case, diagnosis of a specific form of visceral infectious complications is necessary, and the likelihood of developing sepsis is high.
The third option is clearly characterized as sepsis.
Assistance during medical evacuation stages
Tasks:
- Prevention of secondary microbial contamination.
- Elimination of tissue ischemia around the wound.
- Preventing the spread and suppression of pathogens in the wound.
First and first aid
In the yellow zone, the following are particularly important for the prevention of wound infection:
- Applying an aseptic dressing using an Israeli bandage or PPI.
- The use of gentle methods to stop bleeding with maximum preservation of blood flow in the distal parts of the extremities.
- Transport immobilization, incl. for soft tissue injuries.
- Oral antibiotics from a personal first aid kit.
First aid
(measures aimed at preventing infectious complications of wounds):
- Correcting or changing stray aseptic dressings.
- Paravulnar novocaine blockades with high single doses of antibiotics.
- Replacing the tourniquet with another method of temporarily stopping bleeding to reduce limb ischemia.
- Immobilization of the injured limb with standard means (plaster splints, splints).
Surgical methods for treating local infectious complications of wounds:
- Secondary surgical treatment (SDT) of the wound (for secondary indications).
- Complete drainage.
- Early closure of the wound surface.
Features of wound management:
- Use for surgical treatment of wounds complicated by infection, general or regional anesthesia.
For large infected wounds, local anesthesia may not provide sufficient pain relief to remove all nonviable tissue, drain the wound, perform fasciotomy, and place sutures.
- Dissection of the wound should include a wide opening of the fascial sheaths, not only allowing a good view of the wound, but also ensuring the restoration of viable tissues and improving their blood circulation.
- Excision is the main content of VCO. The goal is to ensure the removal of necrotic and non-viable tissue from the wound.
The volume of excision is determined:
- The boundaries of necrosis.
- The boundaries of purulent serous inflammation.
- The type and functional significance of the affected tissues.
- Anatomical and functional feasibility.
- Possibilities of preserving tissue affected by wound infection using conservative treatment.
- The condition of the wounded.
In addition to dead tissue, dense connective tissue affected by the infectious process (areas of tendons, fascia), cartilage tissue and bone must be unconditionally removed. The infectious process in these tissues cannot be stopped using conservative methods.
- Maximum elimination of conditions for colonization and proliferation of microorganisms, suppression of wound infection pathogens by:
a) creating tissue barriers (skin, muscle) between the external environment and tissues with weak resistance to infection.
b) careful hemostasis to prevent the formation of hematomas and closed spaces. An extremely protective attitude towards the skin and a desire to restore the skin as soon as possible is necessary.
- Striving for early wound closure. An indispensable condition for stopping the local infectious process is the restoration of integumentary tissue as a barrier between the external and internal environment.
- Drainage of wounds during VHO:
Passive drainage - the use of gauze swabs and tubular drainages of various diameters. It is used only in the treatment of wounds with minimal signs of wound infection. For the treatment of wounds complicated by wound infection, passive drainage methods are ineffective and often cause direct harm to the wounded, because are quickly accompanied by a cessation of the outflow of wound discharge due to the physical and chemical properties of pus.
Active drainage. Consists of a combination:
- Aspiration of discharge from the wound cavity.
- Constant rinsing of the cavity and wound.
- Direct impact on the wound microflora and the walls of the wound cavity with the help of administered antibiotics, antiseptics and proteolytic drugs. The most effective in treating a purulent wound are silicone double-lumen tubular drainages or several single-lumen drainages that provide active drainage.
The combination of all three elements of active drainage is the best, but requires special equipment. In military field conditions, the simplest and most convenient is long-term active drainage using the “flow method” or vacuum drainage according to Redon.
With any method of drainage, the tube should be placed exactly along the bottom of the purulent cavity and removed through the lowest part of the purulent focus. An important point is the supply of drainage elements through separate punctures, outside the skin wound, because healthy tissues are more resistant to foreign bodies (drainage) and have fewer complications.
Indications for suturing:
- Complete cleansing of the wound from dead and non-viable tissue, achieved by surgical treatment of the infectious focus and conservative treatment.
- Absence of pronounced inflammatory changes in the skin around the wound.
- Possibility of adequate comparison of wound edges without excessive tension. The use of sutures after surgical treatment does not mean applying a “blind” suture to an infected wound. It is necessary to combine a suture of an infected wound with active drainage, ensuring a complete outflow of discharge from the wound cavity. If the edges of the wound are difficult to bring together without tension, then skin grafting with local tissue or free grafting with split flaps is indicated.
Traditional methods of treatment
Minor inflamed cuts and scratches can be treated at home; folk remedies are often used for this.
A hypertonic saline solution (sodium chloride 10%) is suitable for rinsing at the first stage. It can be made at home by adding 90 g of salt to a liter of clean water and straining through sterile gauze. The product draws back and adsorbs exudate without damaging surrounding tissue.
For this purpose, decoctions of chamomile and calendula are also used. A tablespoon of raw material is poured into a glass of water, heated in a water bath for 15 minutes, and filtered thoroughly. Wash the wounds twice a day.
An aloe leaf from an adult plant (at least 2-3 years old) is used as a regenerating and anti-inflammatory agent. It is cut off and placed in the refrigerator for a day. Then they cut it in half lengthwise and tie the inside to the wound.
At the healing stage, mumiyo is used to prevent the formation of a rough scar. 1.5 g of this substance is dissolved in 50 ml of warm water and mixed with a tube of baby cream. Apply once a day. Sea buckthorn oil also helps, it simultaneously softens the skin and stimulates healing.
Remember that traditional methods are applicable only for minor injuries or as an addition to traditional therapy.
Prevention of suppuration
To avoid long-term treatment, you should initially wash and treat all injuries, even minor ones, with an antiseptic. If your doctor has prescribed a wound care procedure, you must follow it and use the prescribed medications. Before dressing, wash your hands thoroughly, use sterile gauze wipes and bandages.
Skin damage due to diabetes and peripheral circulatory disorders does not heal well. In this case, it is recommended to protect yourself from injuries, and if you receive them, seek help from a traumatologist.