Causes
Pathological types of breathing occur for a number of reasons. It is not always possible to accurately determine them, but there are four most common:
- Irritation of the respiratory center associated with the accumulation of toxic metabolic products, hypoxia and increased levels of carbon dioxide, sudden circulatory disorders or intoxications of another nature.
- Acute cerebral swelling due to blunt trauma or compression.
- Damage to the centers of the midbrain and medulla oblongata by a viral infection.
- Strokes or vascular thromboembolism in this area of the brain, accompanied by hemorrhage.
Breathing disorders may be accompanied by symptoms such as confusion and decreased blood pressure.
Physiology of breathing
Breathing is accompanied by alternate inhalation (oxygen consumption) and exhalation (carbon dioxide release). In a short time, many processes occur between them. They can be divided into the following main stages of breathing:
- external (ventilation and diffusion of gases in the lungs);
- oxygen transportation;
- tissue breathing.
External respiration provides the following processes:
- Ventilation of the lungs - air passes through the respiratory tract, is moistened, becomes warmer and cleaner.
- Gas exchange occurs in a short period of cessation of breathing (between exhalation and new inhalation). Alveoli and pulmonary capillaries participate in the exchange. Blood flows through the alveoli into the capillaries, where it is saturated with oxygen and distributed throughout the body. Carbon dioxide is transported from the capillaries back to the alveoli and expelled from the body during exhalation.
The initial stage of breathing promotes the transfer of oxygen from the alveoli into the blood and the accumulation of carbon dioxide in the pulmonary vesicles for further removal from the body.
Bradypnea
Pathological types of breathing, accompanied by a decrease in the number of respiratory movements, develop when the function of the respiratory center is suppressed. This happens when intracerebral circulation is impaired due to a tumor, inflammatory processes (meningitis, encephalitis), rupture of a vessel or pathological accumulation of fluid.
Another reason for slow breathing is severe intoxication. The excitability of the nerve centers located in the spinal cord decreases with an increase in the blood levels of uric acid, acetone, creatinine, insulin, poisons and during infectious-toxic shock.
There are criteria by which doctors determine the presence of bradypnea:
- up to one year - less than thirty breaths;
- up to twelve years - less than twenty respiratory movements;
- from fifty and older – the limit of normal is considered to be up to thirteen breaths per minute.
Transportation and the final result of the exchange
Transportation of gases in the blood occurs thanks to red blood cells. They carry oxygen to organ tissues, where further metabolic processes begin.
Diffusion in tissues characterizes the process of tissue respiration. What does it mean? Red blood cells bound with oxygen enter the tissues and then into the tissue fluid. At the same time, dissolved carbon dioxide moves back to the alveoli of the lungs.
Blood enters the cells through tissue fluid. Chemical processes of breakdown of nutrients are launched. The final oxidation product, carbon dioxide, reenters the blood in the form of a solution and is transported to the alveoli of the lungs.
Regardless of what type of respiration is used by an individual organism, the metabolic processes that occur are the same. The work of the muscles allows you to change the volume of the chest, i.e., inhale or exhale.
Polypnea
Pathological types of breathing, in which the frequency of inhalations increases, occur in patients with fever, anemia, as well as after heavy physical exertion and during pregnancy.
The reason for this state of the body is a decrease in the partial pressure of oxygen in the blood. The reasons for this may be different. From the respiratory system it is:
- inflammatory lung diseases;
- surfactant deficiency;
- chronic obstructive pulmonary disease, emphysema, bronchial asthma;
- acute or chronic pulmonary failure.
From the circulatory system:
- acute or chronic cardiovascular failure;
- anemia;
- carbon monoxide poisoning;
- porphyria and other hereditary blood diseases;
- red bone marrow tumors.
In addition to all the above problems, the level of oxygen in the blood is affected by the process of tissue respiration. Hypoxia irritates the respiratory centers in the medulla oblongata, and the number of respiratory movements increases.
Causes of respiratory dysfunction
Difficulty breathing can be a serious problem for a person. The result of this process is a gradual decrease in the level of oxygen entering the body and, accordingly, placing greater stress on the respiratory system. When breathing is difficult, the body tries to get out of the current situation on its own and strengthens the work of the muscles responsible for inhalation and exhalation. A similar condition is a cause for concern, since it may be a sign of the presence of some pathological process that affects the entire body as a whole.
The reasons for such a process can be varied, ranging from the influence of external factors to the influence of internal criteria. The most common catalyst for the problem is the following conditions that affect the human body:
- the presence of any diseases occurring in the body;
- allergic reactions;
- food and other types of poisoning;
- diabetes;
- physical exercise.
All these reasons can lead to the formation of certain breathing problems, such as rhythm disturbances or an increase in its depth. Each of these conditions can lead to the development of serious diseases that can appear against the background of deteriorating breathing.
Hyperpnea
This type of breathing is not completely pathological; it is observed when metabolism in the body accelerates. Hyperpnea, or hyperventilation, is deep and frequent breathing necessary to better saturate the blood with oxygen, which is needed as a catalyst in metabolic processes.
Most often found in athletes during physical or emotional stress. Pathological conditions include thyrotoxicosis and fever. In some cases, the body does not need as much oxygen, but due to excessive stimulation of the respiratory center, hyperventilation still develops. This situation can lead to a shift in the acid-base balance and an increase in the level of carbon dioxide in the blood.
Be healthy!
The main form of external respiration pathology is respiratory failure. Depending on the nature of the pathological process, acute and chronic respiratory failure are distinguished. In addition, there are three types of respiratory failure:
- obstructive type;
- restrictive type;
- mixed type.
Tachypnea or “breathing of a cornered animal” is rapid shallow breathing (RR over 20 respiratory movements per minute).
Rapid breathing usually occurs when the respiratory center is irritated by waste products of the body (carbon dioxide). Observed in anemia, fever, blood diseases. If desired, it can be caused by an effort of will (hyperventilation), for example, before the expected breath-holding. With hysteria, the respiratory rate can reach 60-80 per minute.
Bradypnea - a pathological decrease in breathing - develops when the excitability of the respiratory center decreases, or when its function is depressed, which can be caused by an increase in intracranial pressure (brain tumor, meningitis, cerebral hemorrhage, cerebral edema) or the impact on the respiratory center of accumulated in significant quantities in blood toxic metabolic products (uremia, hepatic or diabetic coma, some acute infectious diseases and poisoning).
Apnea (lack of breathing) is the absence or cessation of respiratory movements. A pathological process associated with pathology of the respiratory muscles, for example, poisoning with a poison acting like curare or paralysis of the respiratory center, for example, as a result of cerebral edema or traumatic brain injury.
A separate category is obstructive sleep apnea syndrome, which is caused by sagging of the upper airways. This type of apnea usually occurs in people who snore during their sleep and is a poor prognostic sign for the risk of developing acute cardiovascular failure.
The so-called reflex or “false apnea” sometimes occurs when the skin is severely irritated (for example, when the body is immersed in cold water).
Shortness of breath or dyspnea is a violation of the frequency and depth of breathing, accompanied by a feeling of lack of air. In the case of pathological changes in the heart muscle, shortness of breath first appears during physical exertion, and then occurs at rest, especially in a horizontal position (due to an increase in the venous return of blood to the heart), forcing the patient to take a forced sitting position, which promotes the deposition of venous blood from the inferior vena cava system veins in the legs (orthoptic). Attacks of severe shortness of breath (usually at night) with heart disease are a manifestation of cardiac asthma: shortness of breath in these cases is inspiratory (difficulty breathing).
Expiratory shortness of breath (difficulty in exhaling) occurs when the lumen of the small bronchi and bronchioles narrows (for example, with bronchial asthma) or with a loss of elasticity of the lung tissue (for example, with the development of chronic pulmonary emphysema). “Cerebral” shortness of breath occurs with direct irritation of the respiratory center (tumors, hemorrhages and other etiological factors).
Pathological types of external respiration:
- periodic breathing according to the Cheyne-Stokes type - breathing in which superficial and rare respiratory movements gradually become more frequent and deepen and, having reached a maximum on the fifth - seventh breath, weaken and slow down again, after which a pause occurs. Then the breathing cycle is repeated in the same sequence and goes into the next respiratory pause. The name is given by the names of physicians John Cheyne and William Stokes, in whose works of the early 19th century this symptom was first described. The mechanism of pathological Cheyne-Stokes breathing is explained by a decrease in the sensitivity of the respiratory center to CO2: during the apnea phase, the partial tension of oxygen in arterial blood (PaO2) decreases and the partial tension of carbon dioxide (hypercapnia) increases, which leads to excitation of the respiratory center and causes a phase of hyperventilation and hypocapnia (decrease in PaCO2). Cheyne-Stokes breathing occurs normally in young children, sometimes in adults during sleep; pathological Cheyne-Stokes breathing can be caused by traumatic brain injury, hydrocephalus, intoxication, severe atherosclerosis of cerebral vessels, and heart failure (due to an increase in the time of blood flow from the lungs to the brain).
- Large and noisy Kussmaul respirations - deep, rare, noisy breathing, is a form of hyperventilation, often associated with severe metabolic acidosis, in particular, diabetic ketoacidosis, acetonemic syndrome (non-diabetic ketoacidosis) and end-stage renal failure. This type of pathological breathing is named after Adolf Kussmaul, a German doctor who published his research in 1874 and described the appearance of this type of breathing as a sign of coma and imminent death in people with diabetes. Currently referred to in the scientific literature as Kussmaul's symptom - deep noisy rhythmic breathing of an unconscious patient, caused by irritation of the respiratory center with acetoacetic and beta-hydroxybutyric acids. Indicates the presence of metabolic acidosis.
Main types of external respiration disorders:
- alveolar hypoventilation;
- alveolar hyperventilation;
- pulmonary perfusion disorders;
- disturbances in ventilation-perfusion relationships;
- diffusion disorders.
A combination of types of disorders is often observed.
Alveolar hypoventilation
Alveolar hypoventilation is characterized by insufficient alveolar ventilation, resulting in less oxygen entering the blood and usually insufficient removal of carbon dioxide from the blood. Hypoventilation leads to a decrease in the amount of oxygen in the blood (hypoxemia) and an increase in the amount of carbon dioxide in the blood (hypercapnia).
Causes of alveolar hypoventilation:
- airway obstruction;
- reduction of the respiratory surface of the lungs;
- violation of the expansion and collapse of the alveoli;
- pathological changes in the chest;
- mechanical obstacles to chest excursions;
- disorders of the respiratory muscles;
- disorders of central regulation of breathing.
Airway obstructions:
- spasm of small bronchi (obstructive bronchitis, bronchial asthma);
- tongue retraction;
- entry of food, vomit, or foreign bodies into the trachea or bronchi;
- blockage of the newborn's airways with mucus, sputum or meconium;
- inflammation or swelling of the larynx;
- obstruction or compression by a tumor or abscess.
Apnea
Types of pathological breathing in a person can be either with or without stopping. It all depends on the effect on the respiratory center.
For example, this condition can be caused by a decrease in the partial pressure of carbon dioxide in the blood. Natural or artificial hyperventilation can also cause respiratory arrest.
There is also a known symptom of “false apnea,” which occurs due to a sudden change in temperature or difference in air pressure, for example, when falling into cold water. But in this case, respiratory arrest is caused by obstruction of the upper respiratory tract (larynx spasm), and not by a decrease in the functions of the medulla oblongata.
Pathological types of breathing (Cheyne-Stokes, Biot, Kussmaul) have an element of apnea of varying duration.
Types of pathological breathing
There are several types of pathological breathing. The most common are those associated with an imbalance between excitation and inhibition in the central nervous system. This type of illness includes the following types:
- Cheyne-Stokes.
- Kussmaul.
- Grocco.
- Biot's breath.
Each type has its own characteristics.
Cheyne-Stokes breathing
This type of breathing was first described at the end of the nineteenth century, but then doctors were unable to establish the cause of this condition. Doctors associated its appearance with an increase in the level of carbon dioxide in the blood.
Pathological types of Cheyne-Stokes breathing manifest themselves in the form of shallow and rare breaths, which, under the influence of hypoxia, gradually become more frequent and deeper. After seven breaths, hyperventilation occurs and chest excursion slows down again. At the end of the cycle there is a pause, a cessation of breathing, which lasts from five to seven seconds.
This type of breathing is most common in young children and is a variant of the physiological norm. In addition, it develops with head injuries, increased intracranial pressure, cerebral ischemia, poisoning and heart disease.
Breathing disorders
General information
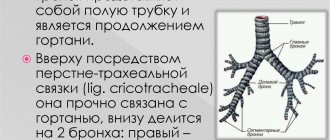
Respiration is a set of physiological processes that provide oxygen to human tissues and organs. Also, during the process of breathing, oxygen is oxidized and removed from the body through the metabolism of carbon dioxide and partially water. The respiratory system includes: nasal cavity, larynx, bronchi, lungs. Breathing consists of stages:
- external respiration (provides gas exchange between the lungs and the external environment);
- gas exchange between alveolar air and venous blood;
- transport of gases through the blood;
- gas exchange between arterial blood and tissues;
- tissue respiration.
You may be interested in: Impaired sense of smell Runny nose
Disturbances in these processes can occur due to illness. Serious breathing problems can be caused by the following diseases:
- Bronchial asthma;
- lung disease;
- diabetes;
- poisoning;
- shock.
External signs of breathing problems allow you to roughly assess the severity of the patient’s condition, determine the prognosis of the disease, as well as the location of the damage.
Causes and symptoms of breathing problems
Symptoms of impaired breathing can be caused by various factors. The first thing you should pay attention to is your breathing rate. Excessively rapid or slow breathing indicates problems in the system. is also important . Rhythm disturbances lead to different time intervals between inhalations and exhalations. Also, sometimes breathing may stop for a few seconds or minutes, and then reappear. Lack of consciousness may also be due to problems in the respiratory tract. Doctors focus on the following indicators:
- Noisy breathing;
- apnea (stopping breathing);
- rhythm/depth disturbance;
- Biota breath;
- Cheyne-Stokes breathing;
- Kussmaul breathing;
- quietpnea.
Let us consider the above factors of breathing problems in more detail. Noisy breathing is a disorder in which breathing sounds can be heard from a distance. Disturbances occur due to decreased airway patency. Can be caused by diseases, external factors, rhythm and depth disturbances. Noisy breathing occurs in the following cases:
- Damage to the upper respiratory tract (inspiratory dyspnea);
- swelling or inflammation in the upper respiratory tract (shortness of breath);
- bronchial asthma (wheezing, expiratory shortness of breath).
When breathing stops, the disturbances are caused by hyperventilation of the lungs during deep breathing. Apnea causes the level of carbon dioxide in the blood to decrease, disrupting the balance of carbon dioxide and oxygen. As a result, the airways narrow and air movement becomes difficult. In severe cases there is:
- tachycardia;
- decreased blood pressure;
- loss of consciousness;
- fibrillation.
In critical cases, cardiac arrest is possible, since respiratory arrest is always fatal to the body. Doctors also pay attention during examination to the depth and rhythm of breathing. These disorders may be caused by:
- metabolic products (slags, toxins);
- oxygen starvation;
- traumatic brain injuries;
- bleeding in the brain (stroke);
- viral infections.
Lesions of the central nervous system cause Biota respiration. Damages to the nervous system are associated with stress, poisoning, and cerebrovascular accidents. May be caused by encephalomyelitis of viral origin (tuberculous meningitis). Biot's breathing is characterized by alternating long pauses in breathing and normal, uniform breathing movements without disturbing the rhythm.
An excess of carbon dioxide in the blood and a decrease in the functioning of the respiratory center causes Cheyne-Stokes breathing. With this breathing head start, respiratory movements gradually become more frequent and deepen to a maximum, and then move on to more shallow breathing with a pause at the end of the “wave”. Such “wave” breathing is repeated in cycles and can be caused by the following disorders:
- vascular spasms;
- strokes;
- cerebral hemorrhages;
- diabetic coma;
- intoxication of the body;
- atherosclerosis;
- exacerbation of bronchial asthma (attacks of suffocation).
In children of primary school age, such disorders are more common and usually disappear over the years. Other causes may include traumatic brain injury and heart failure.
A pathological form of breathing with rare rhythmic inhalations and exhalations is called Kussmaul breathing. Doctors diagnose this type of breathing in patients with impaired consciousness. This symptom also causes dehydration.
The type of shortness of breath called tachypnea causes insufficient ventilation of the lungs and is characterized by an accelerated rhythm. It is observed in people with severe nervous tension and after heavy physical work. It usually goes away quickly, but may be one of the symptoms of the disease.
Treatment
Depending on the nature of the disorder, it makes sense to contact an appropriate specialist. Since breathing problems can be associated with many diseases, if you suspect asthma , consult an allergist. In case of intoxication of the body, a toxicologist will help.
A neurologist will help restore normal breathing rhythm after shock and severe stress. If you have a history of infections, it makes sense to contact an infectious disease specialist. For a general consultation with mild breathing problems, a traumatologist, endocrinologist, oncologist, or somnologist can help. In case of severe breathing problems, you should immediately call an ambulance.
Facebook Youtube Viber Telegram
Kussmaul's Breath
Pathological types of Kussmaul breathing were discovered in Germany at the end of the nineteenth century. The doctor, Adolf Kussmaul, described them in patients with advanced forms of diabetes and presented his discovery as one of the signs of an approaching coma.
Subsequently, scientists found that deep and noisy breathing occurs in other metabolic disorders. Especially with acidosis, that is, a shift in the equilibrium of the environment towards acids. It has been biochemically proven that similar symptoms appear if the respiratory center is irritated by the accumulation of acetoacetic and hydroxybutyric acid.
A decrease in the partial pressure of carbon dioxide and a low concentration of buffer solutions are observed in the patient’s blood.
Depth of breathing.
The depth of breathing is determined by the volume of inhaled and exhaled air. This should be done while the patient is calm. The average tidal volume of an adult is 500 ml. The depth of breathing can increase, such breathing is called deep, or decrease - shallow breathing . Deep breathing is often accompanied by a decrease in breathing , while shallow breathing is often accompanied by an increase. If rare deep breathing is accompanied by a loud noise, then such breathing is called breathing , it is characteristic of a severe coma.
Breath Biota
Pathological types of Biota breathing are also called meningitic breathing. They are characterized by rhythmic, even breathing, interspersed with pauses from thirty seconds to a minute or more.
Most often, this symptom is observed in patients with organic or infectious brain lesions, cerebrovascular accidents, intoxication and shock conditions.
This type of breathing was first described in France in 1876 in a patient with a very severe form of meningitis.
Grokk's Breath
Pathological types of Grokk breathing resemble those of Cheyne-Stokes breathing. This is due to a characteristic change in the depth and intensity of breathing. The only difference is that there is no stop or “pause” at the end of the cycle. When Grokka breathes, it changes to a shallow breath.
In some literature, this type of breathing is called “incomplete Cheyne-Stokes rhythm,” since both symptoms are observed during similar pathologies and may be continuations of each other in the clinical picture of the development of the disease.
What is shortness of breath?
Shortness of breath (in Latin dyspnoe, dyspnea) is difficulty breathing, an altered (compared to normal) state of breathing, manifested as a subjective feeling of constricted, difficult, inadequate breathing.
When shortness of breath occurs, a person wants to take a deeper breath, but tightness in the chest prevents this. There is a feeling of insufficient inhalation, tightness, tightness in the chest, preventing deep breathing. The desire to take a deeper breath becomes obsessive, but unrealizable.
When examining such a patient, the doctor will find objective changes in the main indicators of external respiration function:
- an increase in the minute volume of breathing
due to the depth of breathing (breathing amplitude) and/or its frequency (the number of inhalations and exhalations per minute). Doctors call these phenomena hyperpnea and polypnea. - sudden rapid breathing (tachypnea)
over 40 respiratory acts per minute or - decreased breathing (bradypnea)
- sudden deepening of breathing (batypnea)
or - complete cessation of breathing (apnea)
- small breathing (oligopnea)
- a decrease in the minute volume of breathing due to slowdown (decreasing frequency) - sometimes orthopnea
- a very sharp disturbance in breathing, requiring a forced position for the suffering person to relieve it.
The doctor may also look for rhythm
breathing.
Also officially studied were wave-like breathing, Cheyne-Stokes breathing, Biotian breathing and the breathing that is observed in the dying state - deep Kussmaul breathing
.
So, objectively, outwardly, shortness of breath is accompanied by changes in the depth and frequency of breathing or their ratio, minute volume and rhythm of breathing, and increased work of the respiratory muscles.
From everyday experience it is known that shortness of breath most often occurs during movement or during hard and long work (and in healthy people as well), in the heat or in a stuffy room (for many), with a lack of oxygen in the mountains in people unaccustomed to mountain conditions. Even in a perfectly physically developed athlete, under extreme physical exertion that exceeds the body’s capabilities, breathing can change dramatically, for example, it can become shallow and frequent (lung volume has reflexively decreased), which is felt as squeezing, hardening of the chest (there is a feeling of limited mobility of the chest) or , even, there is a painful feeling of lack of air.
At the same time, with adequate physical activity, all healthy people do not even notice a physiological deepening and/or increased breathing, which does not lead to shortness of breath as a painful symptom.
Apneustic respiration
The chest has limits of extensibility, according to normal physiology. Pathological types of breathing in some cases can shake this truth. When the brain structures responsible for regulating breathing are damaged, an expansion of the chest is observed, which is already in a state of inhalation. The body can no longer regulate the efforts required for breathing movements.
A similar symptom is observed during the dying process of a person. There are successive stages of changes in breathing: dyspnea - respiratory depression - apnesis - gasping breathing, and then paralysis of the respiratory center in the medulla oblongata. This entire cycle is a manifestation of pontobulbar automatism, which develops as a result of inhibition of the activity of higher nerve centers.
When the balance of the internal environment finally shifts towards acids, only isolated sighs and breathing dysrhythmias are observed, which do not fall into any of the above categories.
Gasping breath
The name comes from the English word "gasp", which means gasping for air, or suffocating. This type appears in patients with asphyxia, regardless of its genesis.
Most often, this category of patients includes premature infants, as well as people with closed head injuries and in the stage of severe intoxication. Gasping breathing is characterized by rare breaths of progressively decreasing depth, which are interrupted by pauses in breathing lasting up to twenty seconds. In this case, not only the auxiliary muscles, but also the muscles of the neck and face are involved in the act of breathing.
The initiator of such breathing is the terminal segment of the medulla oblongata, provided that all overlying sections have already ceased to perform their functions.
Types of breathing depending on the nature of respiratory movements
Breathing depends not only on the muscle group involved, but also on indicators such as depth, frequency, and the pause time between exhalation and new inhalation. With frequent, intermittent and shallow breathing, the lungs are not fully ventilated. This creates favorable conditions for bacteria and viruses.
Full breathing engages the lower, middle and upper parts of the lungs, allowing them to be fully ventilated. The entire useful volume of the chest is used, and the air in the lungs is updated in a timely manner, preventing harmful microorganisms from multiplying. A person practicing full breathing takes about 14 breaths per minute. For good ventilation, it is recommended to take no more than 16 breaths per minute.
Dissociated Breathing
In severe disorders caused by damage to the medulla oblongata, “ugly”, “ataxic” breathing is observed. It can be of two types:
- Dissociated. If the patient has paradoxical movements of the diaphragmatic muscles and also asymmetry when lifting the right and left sides of the chest.
- Breathing of Grocco-Frugoni. When there is desynchronization between the intercostal muscles and the human diaphragm.
As a therapeutic tactic for respiratory disorders, transfer of the patient to artificial ventilation with switching off muscle functions by administering muscle relaxants is used. In combination with oxygen therapy, this helps protect the human brain from hypoxia and preserve cognitive function until the normal breathing rhythm is resumed.
The importance of muscles in breathing processes
Types of breathing arose as a result of contraction of the muscles of different parts of the spine. The respiratory muscles provide a rhythmic change in the volume of the chest cavity. Depending on the functions performed, they are divided into inspiratory and expiratory.
The former are involved in the process of inhaling air. The main muscles of this group include: diaphragm, external intercostal, internal intercartilaginous. The accessory inspiratory muscles are the scalenes, pectoralis (major and minor), and sternoclavicular (mastoid). The abdominal and internal intercostal muscles are involved in the process of exhalation.
Only thanks to the muscles is it possible to inhale and exhale air: the lungs repeat their movements. There are two possible mechanisms for changing the volume of the chest through muscle contraction: movements of the ribs or the diaphragm, which constitute the main types of breathing in humans.