general information
Exogenous allergic alveolitis (EAA) is a group of lung diseases that is characterized by diffuse inflammatory changes in the pulmonary tissue. The disease develops after repeated inhalation of allergens.
It is worth distinguishing between two concepts: exogenous allergic and eosinophilic alveolitis. In the first case, a cascade of inflammatory reactions leads to the formation of persistent fibrosis. And with eosinophilic alveolitis, active accumulation of eosinophils occurs in the pulmonary interstitium.
The etiology and clinical picture of these diseases are similar, the difference is found in the persistence of changes, treatment and long-term prognosis. With exogenous allergic alveolitis, the disorders are permanent and not prone to regression. Eosinophilic alveolitis can quickly regress with properly selected therapy.
Lifespan
Life expectancy with exogenous allergic alveolitis depends on the duration of the patient’s contact with antigens, as well as the timeliness of treatment. Life prognosis depends on the stage of development of the disease. In the acute form of EAA, treatment becomes effective and promotes complete recovery (after a month).
In the chronic form, medication measures become ineffective. The development of exogenous allergic alveolitis leads to complications and death. Delayed treatment leads to human disability, which can only be eliminated by lung transplantation.
Without treatment, complications are possible:
- Lack of oxygen;
- Pulmonary hypertension;
- Heart failure as a result of decreased lung performance.
How long do patients with exogenous allergic alveolitis live? It all depends on the stage of the disease and the effectiveness and timeliness of treatment. The more advanced the disease, the shorter people live. On average, life expectancy varies from 3 to 5 years.
Classification
Exogenous allergic alveolitis has many classifications.
By type of flow we can distinguish:
- spicy;
- subacute;
- chronic alveolitis.
Depending on the type of allergen, the disease may be:
- bacterial;
- fungal;
- medicinal (as a result of exposure to drugs);
- caused by antigens of animal origin (serum proteins, animal excrement, bone dust);
- caused by plant antigens (wood dust, pollen, herbal extracts).
Separately, we can distinguish the so-called occupational allergic alveolitis .
These include:
- cheese makers disease;
- farmer's lung;
- bird lovers' lung;
- alveolitis flour millers;
- weavers' cough and others.
Exogenous allergic alveolitis: clinical picture
There are three types of exogenous allergic alveolitis:
- spicy;
- subacute;
- chronic.
Acute allergic alveolitis occurs several hours after contact with the allergen. It is accompanied by fever with chills, cough, shortness of breath, a feeling of heaviness in the chest, joint and muscle pain. Sputum is usually absent, or there is little of it, it is light. Often the patient is bothered by a headache in the forehead. Within two days these signs disappear, but return after new contact with the allergen. In the literature, this phenomenon is called “Monday syndrome”: over the weekend the allergen is removed from the respiratory tract, and on Monday all symptoms recur. Weakness and shortness of breath on exertion persist for a long time. A typical example of an acute course is “farmer's lung”. There is a variant of allergic alveolitis, reminiscent of asthma: after contact with a foreign substance, within a few minutes an attack of suffocation develops with wheezing and the release of viscous mucous sputum. The subacute version of exogenous alveolitis most often occurs during everyday contact with an allergen, for example, among bird lovers. Symptoms are nonspecific: cough with a small amount of sputum, weakness, shortness of breath on exertion. The patient’s life history, hobbies and living conditions play a big role in the diagnosis. With improper treatment, a chronic form of exogenous allergic alveolitis develops. Its onset is imperceptible, but shortness of breath on exertion, weight loss, cardiac and respiratory failure gradually appear and increase. Often the fingers take on the appearance of “drumsticks”, and the nails – “watch glasses”. This sign may indicate an unfavorable prognosis for the patient. The outcome of exogenous alveolitis is “cor pulmonale” and progressive heart failure.
Causes and pathogenesis
The influence of an etiological factor plays a key role in the development of EAA. Moreover, each type of disease is characterized by a specific antigen. Thus, occupational alveolitis can be caused by the following antigens:
| Disease | Allergen |
| Barn disease | Scattered wheat |
| Bagassoz | Moldy sugar cane |
| Disease of those working with wood pulp | Wood dust |
| Weavers cough | Moldy cotton |
| Bird lovers lung | Bird droppings or epidermis |
| Farmer's lung | Rotten hay |
| Suberosis | Cork dust |
In addition to the direct impact factors, predisposing factors are also important. Not everyone who comes into contact with harmful substances suffers from exogenous allergic alveolitis.
The risk group for developing the disease includes:
- smokers;
- persons suffering from chronic diseases of the respiratory system (COPD, bronchitis and others);
- patients with allergic diseases (atopic dermatitis, bronchial asthma);
- long-term ill or weakened persons.
It is worth noting that EAA more often develops in patients at risk, with constant antigenic stimulation of the respiratory tract.
Both immune and non-immune mechanisms play a role in the pathogenesis of EAA. At the initial stage of disease development, a type 3 hypersensitivity reaction occurs. When antigens (fine dust particles, animal or plant peptides) and Ig G interact, immune complexes are formed that damage lung tissue. As a result, the permeability of the vascular wall increases. Formed elements (neutrophils) and inflammatory mediators begin to accumulate in the alveoli (pulmonary vesicles).
In response to this, the protective system of pulmonary macrophages is activated. Exposure to inflammatory mediators and chemotaxis factors enhances necrosis, leading to even greater destruction of lung tissue. All these processes occur within 4-8 hours from repeated contact with the agent.
Stages of exogenous allergic alveolitis
Next, immune T-cell reactions develop (type 4). These changes begin 1-2 days after antigen penetration. Lymphocytes and monocytes begin to rush to the site of inflammation with greater force. Long-term antigenic stimulation causes activation of fibroblasts and the formation of focal granulomas.
More about pneumoconiosis (occupational lung diseases)
Diagnosis.
Acute antigen exposure is often accompanied by neutrophilia and lymphopenia. In all forms of the disease, the erythrocyte sedimentation rate (ESR), levels of C-reactive protein, rheumatoid factor and serum immunoglobulins may increase. Antinuclear antibodies are rarely detected.
Analysis of serum precipitins to expected antigens is an essential part of the diagnostic workup. They indicate the body’s immunological reaction to the influencing antigen. However, it is impossible to diagnose the disease using this criterion alone, since it allows one to judge only the quantity and type of antigen. Precipitins are found in the serum of many individuals exposed to the antigen, but without signs of allergic alveolitis. False-negative results may be due to poor quality of antigens and inappropriate selection. It is recommended to isolate antigens from the surrounding air.
The chest x-ray shows no typical signs. Changes in it are not detected even in patients with obvious symptoms of the disease. In acute and subacute forms, fuzzy spots, diffuse or individual nodular infiltrates may be visible; in the chronic form, a network of diffuse nodular infiltrates appears. The cellularity and reticulation of the pulmonary pattern indicate the progression of the disease. Patients rarely present with disorders such as pleural effusion, induration, or hilar adenopathy.
Functional pulmonary tests in all forms indicate a decrease in lung volume, impaired diffusion capacity, decreased elasticity, and hypoxia during physical activity. Depending on the severity of the disease, residual hypoxemia may be detected. Functional impairment may gradually worsen or develop rapidly with acute or subacute exposure to the antigen. Important criteria for the progression of the chronic form of the disease are changes indicating airway obstruction. For diagnostic purposes, sometimes they resort to bronchoalveolar lavage (the characteristic signs of the lavage fluid have already been mentioned).
A lung biopsy is indicated if other criteria are insufficient to make a diagnosis. It is usually initially performed transbronchially, but in some cases there is a need for an open biopsy, since it provides more adequate data. Although histological changes are quite typical, they are not pathognomonic. If a biopsy is obtained in the active phase of the disease, it reveals an interstitial alveolar infiltrate consisting of plasma cells, lymphocytes, sometimes eosinophils and neutrophils, and granuloma. As a rule, interstitial fibrosis is detected, but in the early stages of the disease it is mild. Almost half of the patients have bronchiolitis, while vasculitis is not a hallmark of the disease. Due to the lack of standard non-irritant antigens and validated data, skin and inhalation tests are useful for experimental purposes only. Similarly, tests for cell-mediated (delayed) hypersensitivity are not indicated.
Symptoms
The clinical picture of the disease depends on the type of aggressive factor, its concentration and duration of contact. With massive exposure to the antigen, an acute form of EAA develops.
It is characterized by the following symptoms:
- chills;
- fever;
- cough;
- dyspnea;
- thoracalgia (chest pain);
- painful sensations in joints and muscles;
- nausea;
- weakness.
Objectively, it is possible to identify symptoms of massive intoxication and severe respiratory failure. Auscultation initially reveals hard breathing, which is soon replaced by variable wheezing sounds in various parts of the lungs.
When contact with the antigen is stopped, symptoms disappear within 1-2 days. With continued exposure, a subacute form of the disease develops. Symptoms become more persistent, but their severity decreases. Signs of intoxication and asthenia are increasing. Patients rapidly lose weight and are troubled by fatigue and exercise intolerance. Auscultation reveals scattered crepitus and isolated dry rales.
The chronic form of EAA develops with prolonged and systematic contact with the antigen. The clinical picture is dominated by signs of respiratory failure. Exercise intolerance, cachexia, malaise, weakness and an unproductive cough are also observed. Fever is rare. The auscultatory picture is also nonspecific: signs of bronchial obstruction, single or multiple wheezing, crepitus.
The clinical picture of exogenous allergic alveolitis is extremely vague.
Diagnosis of exogenous allergies
If differential diagnosis is difficult (with chronic alveolitis), lung tissue biopsy and histology are indicated
To identify the disease, a method is often used to determine precipitating antibodies to a specific antigen, if it is believed that it was contact with it that caused the manifestation of exogenous allergic alveolitis. Even if research reveals high titers of antibodies to an antigen, it can be considered as a provocateur of the disease only if there is other evidence. We are talking about clinical symptoms, X-ray data, and functional manifestations of the disease. In approximately 30% of practically healthy people exposed to the same antigen, precipitating antibodies will be detected in laboratory titers, so their presence alone does not allow us to draw serious conclusions.
To clarify the diagnosis, a provocative test is prescribed. The essence of the technique is to place the patient in an environment where he fell ill, and carefully monitor his health status at this time. The need for a provocative test arises especially seriously when the doctor suspects that the cause of the patient’s illness may be hidden in the air conditioner or humidifier - such household appliances become a breeding ground for harmful bacteria if not cleaned regularly. Not everyone is recommended to undergo a provocative test, as this can lead to a deterioration in the patient’s well-being.
The doctor should prescribe a differential diagnosis with alveolar cancer, signs of miliary tuberculosis, sarcoidosis and other similar pathologies. For example, with cancer of the lung tissue, in contrast to exogenous alveolitis, there is no clearly visible connection between the current condition and the exogenous allergen. X-ray signs will also differ; precipitating antibodies to allergens will not be detected in the blood.
With miliary tuberculosis, unlike alveolitis, there is no connection with external antigens, the disease takes longer and is more severe, and X-ray data are different. In addition, with tuberculosis, a positive serological and skin reaction with tuberculosis antigen is detected; no increase in the titers of precipitating bodies to exoallergens is found in the blood. Sarcoidosis will differ from exogenous alveolitis by test data and x-rays, enlarged lymph nodes, changes in the eyes, joints, etc.
If differential diagnosis is difficult (with chronic alveolitis), lung tissue biopsy and histology are indicated.
The diagnosis of toxic-allergic alveolitis is made based on the identified facts:
- the sanitary and hygienic characteristics indicate working conditions to indicate probable contact with a specific antigen;
- shortness of breath and dry cough, general malaise, temperature rise above 38 degrees after a couple of hours from contact with the antigen. All symptoms disappear a couple of hours after contact with the irritant is interrupted;
- auscultatory and objective data, auscultation over the lungs of 2-sided crepitus;
- information from a pulmonologist and allergist;
- results of instrumental examinations;
- laboratory test data (increased levels of TNF-b, ESR, interleukin-8, C-reactive protein, IgG and IgM).
In addition to the listed factors, allergic alveolitis is indicated by a decrease in lung volume during restrictive ventilation disorders. The doctor may notice forced exhalation in the patient, physical activity causes hypoxemia, and prick tests give a positive result, as does a provocative inhalation test.
The X-ray shows a strong darkening of the pulmonary field, small focal shadows and a reticular nodular lesion are formed. All of these symptoms go away over time if contact with the irritant is eliminated.
If the disease occurs in acute and subacute forms, then the pulmonary fields on x-rays look like frosted glass, fuzzy spots and nodular infiltrates appear. The chronic form is characterized by the appearance of pleural effusion, a continuous network of nodular infiltrates.
Scintigraphy is almost never used for diagnosis because it does not provide correct information regarding EAA. But you can use bronchoalveolar lavage, which allows you to detect a 5-fold increase in T-lymphocytes. During the procedure, foamy macrophages are visible on the lung.
If the listed diagnostic methods are not enough for the doctor to determine the final diagnosis, you can resort to a biopsy. Allergic alveolitis is often accompanied by peribronsial inflammatory infiltrates. Three morphological signs allow one to identify EAA: alveolitis, bronchiolitis and granulomatosis. Whatever the form of exogenous allergic alveolitis, treatment is carried out in each case.
Diagnostics
The diagnosis of “exogenous allergic alveolitis” is established on the basis of anamnestic (presence of a source of antigens in everyday life or at work) and clinical (symptoms of the disease) data, as well as the results of laboratory and instrumental studies.
When conducting laboratory tests, more attention should be paid to general and biochemical blood tests. EAA is characterized by leukocytosis. The degree of its severity depends on the stage of the disease. A “leukocyte peak” is observed in acute cases. Along with an increase in the number of leukocytes, an acceleration of ESR, an increase in eosinophils and a shift of the formula to the left can be observed.
A biochemical study reveals an increase in the level of immunoglobulins G, M, A. An increase in the activity of rheumatoid factor is also possible. An increase in the level of LDH (lactate dehydrogenase) indicates an active destructive process in the lung tissues.
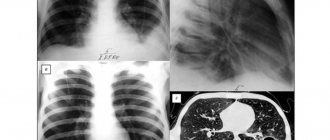
X-ray of a patient with EAA
X-ray examination of the chest organs is the main instrumental method for diagnosing EAA. It is easy to use, accessible and cost-effective. In addition, specific changes are clearly visualized in the image.
At the onset of the disease, most often the pathology cannot be detected. Occasionally, you can see the “frosted glass” phenomenon: a decrease in the transparency of the lung fields. As the disease progresses, nodular reticular opacities are detected. In this case, the size of the shadows does not exceed 0.3 cm in diameter.
In the chronic course, clear linear shadows and nodular darkening are visualized. In severe cases, you can see the so-called “honeycomb lung”: alternating areas of darkening and clearing.
Computed tomography is considered a more sensitive diagnostic method. It is prescribed if the initial stage of the disease is suspected and in the absence of characteristic changes on the x-ray.
CT scan of exogenous allergic alveolitis
External respiration testing is most often used as a functional test. In the acute stage, a restrictive type of breathing disorder can be identified. At the same time, the total and vital capacity of the lungs, functional residual capacity and functional residual volume decrease. The Tiffno index is within normal limits.
In the chronic form, a decrease in static indicators is observed. Examination may reveal signs of severe obstruction or emphysema.
The most specific indicator is the diffusion capacity of the lungs. Its decrease is the first sign of the disease. Studying this indicator over time can objectively show a change in the patient’s condition.
Provocative tests involve inhalation of an aerosol that contains specific antigens. In sensitized individuals, this procedure causes an asthma-like attack. This method is not popular due to its non-specificity and lack of technical equipment. Provocative tests can only be used to confirm the etiological nature of the disease.
Course of the disease.
The clinical picture is individual and depends on the frequency and intensity of exposure to the antigen, as well as on other characteristics of the body. There are acute, subacute and chronic allergic alveolitis. In the acute form, cough, fever, chills, malaise and shortness of breath appear 6-8 hours after exposure to the antigen and usually disappear after a few days if its exposure stops. The subacute form occurs insidiously for several weeks after exposure, manifesting as cough and shortness of breath, and may progress to the appearance of cyanosis and respiratory failure, which requires hospitalization of the patient. Sometimes a subacute form can develop after an acute one, especially with continued exposure to the antigen. In many patients with acute and subacute forms, subjective and objective signs of the disease disappear several days, weeks or months after the cessation of exposure to the harmful factor. Otherwise, the disease may become chronic, but the frequency of such transformation is unknown. The chronic form of the disease can be represented by gradually progressive interstitial lung disease, accompanied by cough and shortness of breath during exercise, without previous manifestations of the acute or subacute form. The gradual onset of the disease usually occurs when exposed to low doses of antigen.
Treatment
The main point in the treatment of EAA is the elimination of interaction with the etiological agent - the allergen. If the disease is related to work activity, it is necessary to create conditions for the patient in which contact with the agent will be minimal.
As conservative therapy, immunosuppressive drugs and drugs that correct oxygen deficiency are used.
Glucocorticosteroids are effective in all forms of EAA. They reduce inflammation and reduce the degree of fibrosis of lung tissue. Depending on the nature of the disease, therapy can last from 3-4 weeks to several years. In the chronic form, the effects of steroids are less pronounced. Systemic hormonal drugs are used as basic therapy ; however, in order to avoid side effects, it is permissible to prescribe local treatment at the stage of maintenance therapy.
In general, read about the treatment of alveolitis here
In case of significant disturbances of the immune status, the use of cytostatic drugs is possible. They are also able to slow down the progression of the disease and lead the patient to stable remission. However, this treatment tactic is rarely used due to the small number of studies.
As symptomatic treatment, bronchodilators are prescribed (in case of development of obstructive syndrome) and oxygen therapy (in the presence of severe respiratory failure).
If therapy is ineffective and the disease progresses rapidly, surgical treatment is resorted to. Patients undergo donor lung transplantation. It must be taken into account that upon repeated contact with the allergen, a relapse of the disease often occurs in the transplanted lung.
Expert opinion
Lyudmila Sokolova
Pediatrician, doctor of the highest category
Ask a Question
Treatment of EAA in children is carried out according to the same clinical recommendations. The dose is calculated based on the child’s body weight and the severity of symptoms.
Treatment of allergic alveolitis
Therapy is prescribed depending on the form of the disease and the severity of clinical manifestations.
In the acute course of the pathology, to relieve symptoms, it is often enough to interrupt the patient’s contact with the etiological factor. But this is only effective if the patient has been in contact with the allergen for just a few hours.
When allergic agents affect the human body for a long time and the contact is massive, then drug treatment will be required to eliminate the clinical manifestations. Drug therapy begins with taking corticosteroids. They allow you to quickly get rid of an allergic reaction and eliminate inflammation.
In the acute phase, the following drugs are prescribed:
- Prednisolone.
- Azathioprine.
- Cuprenil.
When choosing initial doses and course duration, the doctor takes into account the presence of concomitant diseases in the patient, his age and body weight, and the severity of symptoms. In the acute form of the disease, the course of hormonal drugs lasts for a month. The subacute form requires a longer course. Hormonal corticosteroids are discontinued after the patient's condition has stabilized. They are being replaced by bronchodilators and antihistamines. In the chronic course of the pathology, the patient is prescribed drugs that improve the functioning of the heart muscle.
Reference materials (download)
| # | File | file size |
| 1 | Professional exogenous allergic alveolitis. Clinical recommendations.MZRF.2019 | 971 KB |
| 2 | Exogenous allergic alveolitis. Differential diagnostics (manual for doctors). 2013 | 899 KB |
| 3 | Professional exogenous allergic alveolitis. Clinical recommendations.MZRF.2019 | 971 KB |
| 4 | Hypersensitivity pneumonitis (exogenous allergic alveolitis) in children (diagnosis and treatment). Clinical guidelines | 969 KB |
| 5 | A case of recurrent variant of exogenous allergic alveolitis | 231 KB |
| 6 | Clinical case of difficulty in diagnosing exogenous allergic alveolitis | 346 KB |