| Reye's syndrome | |
| ICD-10 | 93.793.7 |
| ICD-9 | 331.81331.81 |
| DiseasesDB | 11463 |
| MedlinePlus | 001565 |
| eMedicine | emerg/399 |
| MeSH | D012202 |
Reye's syndrome
,
Reye's syndrome
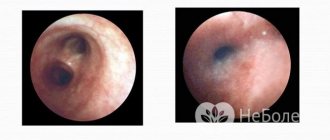
(acute liver failure and encephalopathy, “white liver disease”) is a rare but very dangerous, often life-threatening acute condition that occurs in children and adolescents (usually aged 4-12 years) during treatment of viral fever origin (influenza, measles, chickenpox) with drugs containing acetylsalicylic acid, and is characterized by rapidly progressing encephalopathy (due to cerebral edema) and the development of fatty infiltration of the liver. Reye's syndrome is accompanied by hyperammonemia, increased levels of AST, ALT in the blood serum (more than 3 times) with normal bilirubin levels.
Reye's syndrome is based on generalized mitochondrial damage due to inhibition of oxidative phosphorylation and impaired β-oxidation of fatty acids.
The syndrome was first described by Australian pathologist Douglas Reye in 1963[1].
What is Reye's syndrome?
Reye's syndrome (white liver disease) is an acute condition that occurs in childhood or adolescence after the use of drugs containing acetylsalicylic acid to reduce fever during viral infections, such as:
- flu;
- chicken pox;
- measles.
It is life-threatening in nature, manifested by cerebral edema, leading to encephalopathy, as well as acute liver failure due to the development of fatty infiltration of the liver.
Reasons for the development of the disease
The disease was first described by Australian pathologist Douglas Rye in 1963, but the exact mechanism of development of the syndrome has not yet been elucidated.
It is known that it is based on mitochondrial damage, which is of a generalized nature.
It occurs as a result of inhibition of oxidative phosphorylation, as well as disruption of fatty acid oxidation.
It has been noted that the development of Reye's syndrome is preceded by the use of salicylates against the background of a viral pathology. The decline in aspirin use in the 1980s in Anglo-Saxon countries led to a decrease in reported cases of the disease.
Children suffering from a disorder of fatty acid oxidation are more predisposed to the development of this pathology and are at risk for Reye's syndrome.
Symptoms in children
The first manifestations of the syndrome are observed on the 4-5th day of chickenpox, or 5-6 days after the development of other viral infections.
The main clinical signs at the initial stage are nausea and uncontrollable vomiting.
During this period of illness, they can be mistaken for symptoms of an intestinal infection or flu with abdominal syndrome.
With white liver disease, 24-48 hours after the onset of vomiting, the primary manifestations are accompanied by a change in the child’s mental state, which can have various options:
- slight lethargy;
- episodes of disorientation;
- psychomotor agitation;
- irritability;
- aggressive behavior.
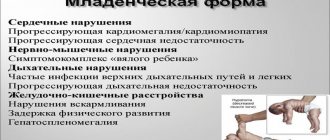
This is followed by rapid breathing and paralysis of individual muscle groups.
In children under one year of age, tension in the large fontanel is observed. Manifestations of the disease in children under 3 years of age are often respiratory dysfunction, drowsiness, and seizures.
If adequate medical care is not provided in time, a rapid deterioration of the condition occurs, with the progression of depression of consciousness. Decerebrate and decortication postures are characteristic. In the first case, the child's arms and legs are straightened, their fingers point down, and their head and neck are tilted back. The muscles tense. This body position indicates serious brain damage.
Decortication pose involves flexion and supination of the arms and extension of the legs.
This body position indicates bilateral damage to the cerebral hemispheres, which leads to separation of the cortex and brain stem.
The basic vital functions of the body are disrupted: respiratory arrest occurs, cardiovascular failure, and coma develop.
One of the symptoms of the disease is thrombohemorrhagic syndrome, which can manifest itself as a minor petechial rash, or (in a complicated version) heavy bleeding.
The prognosis of the disease depends on several factors:
- the rate of progression and severity of changes in brain function;
- indicators of intracranial pressure;
- ammonia content in the blood, indicating the degree of inhibition of liver function.
Complications of Reye's syndrome are:
- mental retardation;
- seizure disorders;
- damage to nerve endings in the periphery.
The mortality rate for this disease usually ranges from 20 to 30%, but if the course of the syndrome is mild, it does not exceed 2%. The onset of deep coma leads to the death of more than 80 children out of a hundred.
Children who have had Reye's syndrome should be referred for genetic counseling to rule out the presence of congenital metabolic diseases.
Predictions for Reye's syndrome
Only quick diagnosis and timely therapy are the basis for a successful outcome of the disease. Recently, the mortality rate of patients diagnosed with Reye's syndrome has decreased markedly, but infants and patients in stage 4 of the pathology in question are exceptions.
If we talk about the prognosis of the disease, it depends only on the degree of changes in the functions of the central nervous system and the rate of progression of disorders. If the patient has overcome the acute phase of the pathology, then in most cases there is a complete recovery. In some cases, signs of damage to brain cells may appear - for example, a child begins to experience mental retardation, periodic seizures, and pathologies of peripheral nerves.
An unfavorable prognosis for Reye's syndrome has its own distinctive features - the patient experiences a rapid change in the first three stages, seizures appear at an early stage, and intracranial pressure increases sharply.
Please note: Reye's syndrome almost never develops twice in the same person. Doctors also cannot yet explain this fact.
Of course, it’s worth knowing the rules for preventing Reye’s syndrome - such a disease is definitely easier to prevent than to treat later. Firstly, you need to carefully monitor the health of a child or adult who is at the stage of developing a viral infection. At the first manifestation of problems in the functioning of the gastrointestinal tract, you should immediately seek qualified medical help, and not self-medicate. Secondly , it is necessary to exclude acetylsalicylic acid preparations (Aspirin, in particular) from the treatment of viral infections.
Reye's syndrome is a dangerous and “insidious” disease. Yes, it is rare, but it can develop in every child and adult against the background of ongoing viral infections. Modern medicine is able to help patients with the pathology in question, but for this it is necessary to carry out timely diagnosis. And given the likelihood of complications developing against the background of brain damage, it will be much easier to take the necessary preventive measures and avoid the development of Reye's syndrome.
Tsygankova Yana Aleksandrovna, medical observer, therapist of the highest qualification category
9, total, today
( 50 votes, average: 4.44 out of 5)
Biliary dyskinesia - causes, symptoms, forms and treatment methods
Yellow coating on a child’s tongue: causes and treatment
Related Posts
Diagnosis of the disease
It is difficult to diagnose Reye's syndrome in a child due to the lack of a specific test to determine this condition.
Differential diagnosis is carried out excluding the following diseases:
- neuroinfections such as encephalitis, meningitis;
- acute hepatitis;
- sepsis;
- poisoning;
- inborn errors of metabolism.
A history of taking salicylates or other sources of mitochondrial toxins helps to suspect Reye's syndrome.
Blood tests (general and biochemical) are required. In some cases, the number of leukocytes is higher than normal. There is a decrease in sugar, a pathognomonic sign is a sharp increase in ammonia levels. The amount of bilirubin remains within acceptable limits, although liver enlargement is observed in 40% of cases. AST and ALT exceed the norm by more than 3 times.
Disruption of the coagulation system is reflected in the results of the coagulogram.
Tests are performed to identify disturbances in the oxidation of fatty acids, as well as other metabolic processes in the body.
Required examinations:
- electroencephalogram;
- ultrasound examination of the abdominal organs, revealing hepatomegaly, its structural compaction and increased echogenicity;
- CT scan;
- MRI;
- puncture of the cerebrospinal fluid, which allows to exclude an infectious-inflammatory cause of encephalopathy;
- liver biopsy confirming signs of fatty degeneration.
Complications and consequences
The disease is characterized by rapid development and severe course .
If the child is not provided with timely medical care, dangerous complications may develop, such as coma, cirrhosis of the liver, persistent convulsive syndrome, mental and intellectual development disorders.
In particularly difficult situations, the likelihood of a child's death is high . Other complications include:
- disturbances in the functioning of the cardiovascular system up to complete cardiac arrest;
- asphyxia;
- pancreatitis, accompanied by death of pancreatic tissue;
- blood poisoning (sepsis);
- development of pneumonia;
- paralysis of arms or legs;
- hemorrhages in the gastrointestinal tract.
Treatment of Reye's syndrome
The disease cannot be treated at home. Hospitalization is required, in some cases in the intensive care unit.
Constant monitoring of the state of the central nervous system, heart function, breathing, water and electrolyte balance, and intracranial pressure is required.
Arterial catheterization is used to study the gas composition of the blood and its pH.
Treatment of the syndrome is aimed at maintaining the vital functions of the body.
Correction of acidosis, hypoglycemia, and hyperammonemia is necessary. Saline solution, glucose, and vitamin K are injected intravenously. In case of severe thrombohemorrhagic syndrome, an infusion of plasma and platelets is necessary.
Treatment of seizures is carried out with the help of Phenytoin; Metoclopramide and Cerucal are used to combat vomiting. Diuretics are used to reduce intracranial pressure. Prescribe Mannitol 0.5-1.0 g/kg intravenously in an age-specific dosage.
In severe cases, tracheal intubation and artificial ventilation are required.
Disease prevention
Screening of newborns for the presence of pathology associated with impaired fatty acid oxidation helps to identify a group at risk for Reye's syndrome.
Caution must be exercised when prescribing drugs containing acetylsalicylic acid to children under 12 years of age for the treatment of hyperthermia due to viral infections.
In these cases, the use of medications such as paracetamol and ibuprofen is recommended.
In order not to make a mistake in choosing a drug to reduce fever, it is important to consult with a pediatrician and also carefully study the composition of the chosen medicine.
If you suspect Reye's syndrome, you must immediately call an ambulance!
When treating a viral infection in a child, it is important to remember the possibility of such a dangerous condition as white liver disease. Do not use aspirin-containing medications to reduce high fever. If it is necessary to use such medications, it is important to carefully monitor the child’s condition.
epidemiology
Reye's syndrome occurs almost exclusively in children.
Although some adult cases have been reported over the years, these cases usually do not show permanent neural or liver damage. Unlike the UK, surveillance for Reye's syndrome in the US is focused on patients under 18 years of age. In 1980, after the CDC began warning doctors and parents about the association between Reye's syndrome and the use of salicylates in children with chickenpox or virus-like illnesses, the incidence of Reye's syndrome in the United States began to decline. However, the decline began before the FDA's release of a warning label on aspirin in 1986. In the United States, between 1980 and 1997, the number of reported cases of Reye's syndrome decreased from 555 cases in 1980 to about 2 cases per year since 1994 .
during this time period, 93% of reported cases for which racial data were available occurred in whites and the average age was six years. In 93% of cases, this viral disease occurred within the previous three weeks. For the period 1991–1994, the annual hospitalization rate for Reye's syndrome in the United States was estimated to range from 0.2 to 1.1 per million population less than 18 years of age.
A 1980 case-control study carried out in the United Kingdom also demonstrated an association between Reye's syndrome and aspirin exposure. In June 1986, the United Kingdom's Committee on the Safety of Medicines issued warnings against the use of aspirin in children under 12 years of age and warning labels were introduced on aspirin-containing medicines.
From November 1995 to November 1996 in France, a national study of pediatric wards of children under 15 years of age with unexplained encephalopathy and a threefold (or more) increase in serum aminotransferase and/or ammonia resulted in the identification of nine definite cases of Ryomo syndrome (0.79 cases per million children).
Eight out of nine children with Reye's syndrome were found to have been exposed to aspirin. In part because of this survey result, the French drug agency has increased international attention to the relationship between aspirin and Reye's syndrome, issuing its own government and professional warnings about this relationship.